The Emigration of Medical Doctors from Albania: Brain Drain vs Return and Cooperation
-
Author(s):Gëdeshi, IlirKing, RussellCeka, AmarildoPublished in:Central and Eastern European Migration Review, Vol. , No. online first, 2024, pp. 1-21DOI: 10.54667/ceemr.2024.16Received:
30 April 2024
Accepted:31 October 2024
Published:19 November 2024
Views: 504
Across many countries of Central and Eastern Europe the emigration of skilled professionals since 1990 has become a serious problem of the loss of specialised human capital. This paper on Albanian doctors is one of the first to study in depth an example of this broader phenomenon of brain drain from the CEE region. There is a global demand for medical doctors which exceeds supply, leading to international competition in which the richer countries, with higher salaries and better working conditions, attract medical graduates and trained doctors from poorer countries. The migration of doctors from Albania is set within this globalised and hierarchised market for medical expertise. On the one hand, the movement of doctors to richer countries helps to plug the deficit in their supply in such countries and enables the individuals concerned to improve their incomes and life conditions. On the other hand, the loss of medical professionals severely harms the structure and quality of the health service in the sending country. This paper addresses three main questions. First, what are the characteristics of the Albanian medical brain drain in terms of its size, socio-demographics and destination countries? Second, what are the causes and consequences of Albania’s loss of medical doctors? Third, what are the prospects of the migrant doctors returning to Albania or contributing their expertise from abroad? Answers are provided via a dual methodology of an online survey of Albanian doctors currently working abroad (N=301) and follow-up interviews with 25 of them. More than half of the survey respondents do not intend to return to Albania and a further third are undecided. Interview data indicate that the doctors are well-integrated abroad and see ‘no future’ for themselves and their families in Albania. There is, however, a greater willingness to share expertise with the home country via cooperation and short visits. Obstacles to return are partly income-related but, to a greater extent, reflect the poor working conditions and career prospects in Albania, including endemic corruption – the same factors that caused emigration in the first place. The policy implications of our findings are challenging; one solution is to mandate a period of work in Albania for newly qualified doctors before they are allowed to go abroad.
Introduction and context
At both a European and a global level, there is a systemic shortage of trained health professionals, including medical doctors, who form an important niche in the globalised market for highly skilled labour (Adovor, Czaika, Docquier and Moullan 2020; Grignon, Owusu and Sweetman 2013). This global and regional supply–demand inequality leads to an ‘unhealthy’ competition for doctors in which the winners are the richer countries, which are able to offer high salaries and good working conditions – and the losers are poorer countries which suffer from a medical brain drain. Is it fair, one may ask, that a relatively poor country like Albania should fund the upbringing and expensive training of medical graduates, only for those highly educated individuals to be lured to rich countries like Germany or the United States to remedy the insufficient supply of home-grown doctors? Is this not a form of development assistance given by poor to rich countries and therefore fundamentally unjust? (King 2018).
These questions have particular poignancy when we consider that doctors, nurses and other health professionals do the most vital job imaginable – they sustain and restore human life. Yet the training of doctors is longer, more demanding and more expensive than just about any other profession and entry requirements for admission to medical schools are amongst the highest of all tertiary-level subjects. Hence, we argue that the ‘brain drain’ of doctors is uniquely problematic, exacerbating already existing health-service inequalities between rich and poor countries located respectively in the global North and global South or, within Europe, between ‘West’ and ‘East’. At the same time, we acknowledge the innate tension between, on the one hand, the individual’s right to migrate and seek self-improvement and, on the other, the structural injustices in the geographical distribution of the costs and benefits of training and employing doctors, nurses and other health professionals.
Like all segments of the labour market, the competition for medical doctors is determined by the interaction of supply and demand (Buchan, Campbell, Dhillon and Charlesworth 2019; Grignon et al. 2013; Kroezen, Dussault, Craveiro, Dieleman, Jansen, Buchan, Barriball, Rafferty, Bremner and Sermeus 2015; Tajdens, Weilandt and Eckert 2012; Wismar, Maier, Glinos, Bremner, Dussault and Figueras 2011). Given the situation of overall shortage, the market is mainly demand-driven. The key demand factors are demographic: ageing populations, especially in Europe and North America with the retirement of the baby-boomer generation born in the early postwar years; rising life expectancy due to medical advances and more-healthy lifestyles; and the need to recruit more medical staff to support the continued advances in treatment and research. Also noteworthy is the ageing of doctors, one third of whom were aged over 55 in the EU in 2020 (Mara 2020). Consequently, most European and OECD countries report chronic shortages of doctors and other medical personnel (Kroezen et al. 2015; Mara 2020; OECD 2019; Wismar et al. 2011).
The supply side of the labour market is characterised by the insufficient production of young doctors in many advanced countries and hence the existence of many unfilled vacancies and the policy of recruiting doctors from other countries. One result is the growth in enrolment for medical degrees in poor countries, in response to the high salaries and good career prospects abroad. This raises important ethical and moral questions over the extent to which richer countries are exploiting poorer ones in the competition for trained doctors and medical graduates (Glinos 2015; Mara 2020, 2023). On the other hand, the ‘beneficial brain drain’ hypothesis argues that the incentive of higher incomes through emigration stimulates overall entry into higher education and training, thereby improving the stock of human capital in the source country net of emigration (Commander, Kangasniemi and Winters 2004; Docquier and Rapoport 2012).
As well as the more obvious supply and demand drivers, there are numerous individual and conditioning factors which shape the migration of doctors and other health-service personnel. The individual-scale elements include classic socio-economic ‘push and pull’ factors – such as low earnings and poor living standards in the country of origin and higher incomes and a better quality of life abroad. The conditioning factors consist of facilitating/discouraging elements such as spatial distance, language knowledge, the culture of the destination country, visa issues, the possibility to take dependents and, more specific to professional and highly skilled migrants, the recognition of qualifications. Mara (2023) analysed some of these factors influencing the migration of health professionals from the Western Balkans to the richer countries of Europe, especially Germany. Her gravity-model analysis confirmed the importance of income differentials in explaining mobility patterns, as well as geographical proximity and institutional/policy factors such as the German ‘special regulation’ introduced at the end of 2015 facilitating the immigration of health professionals from Albania and other countries of the Western Balkans. In fact, the European scenario comprises complex chains of migration and replacement migration, so that even some advanced countries ‘lose’ their doctors and health professionals to richer countries where salaries and working conditions are better – for instance, from Germany to Switzerland, from Sweden and Finland to Norway and from the United Kingdom to Canada, Australia and New Zealand. At the bottom of the chain of supply are countries like Albania, Kosovo and Bosnia and Herzegovina, which train and then ‘give’ their doctors to Germany and other wealthy countries. Our paper advances Mara’s (2023) quantitative exploration of the emigration of health professionals from the wider Western Balkan region by an in-depth focus on the emigration of doctors from one country, Albania, employing a mixed-methods approach combining an online survey with qualitative interviews.
Focusing more specifically, then, on Albania, the population there, too, is rapidly ageing. According to the Albanian Census of 2023 (INSTAT 2024), the share of the population aged 65+ almost tripled over the past 22 years, increasing from 7.5 per cent of the total in 2001 to 19.7 per cent in 2023. This share will undoubtedly continue to grow because of increasing longevity, a declining birth rate (down to 1.3 children per woman in the early 2020s) and the still-ongoing emigration of younger-age cohorts, which also removes some of the future reproductive potential of the Albanian population.
Two other important segments of contextual information complete this Introduction: the massive relative scale of Albanian migration and the parlous state of the Albanian health system. Since 1990, Albania has experienced one of the largest emigrations, relative to the size of its population, in the world. Emigration has dramatically reduced the Albanian population from 3.2 million at the last communist-era census (1989) to 2.4 million at the 2023 census. Between the two most recent censuses (2,831,741 in 2011; 2,402,113 in 2023), the population shrank by nearly 15 per cent (INSTAT 2024). Migration abroad, coupled with intense internal migration, has infused every sector of the Albanian society, economy and landscape; few families or places remain unaffected (Vullnetari 2012). International bodies such as the World Bank (2016) and OECD (d’Aiglepierre, David, Levionnois, Spielvogel, Tuccio and Vickstrom 2020) rank Albania amongst the top countries globally both for the ratio of its ‘stock’ of emigrants to the resident population (around 40 per cent) and for the relative scale of its brain drain as a share of total emigration in the period 2011–2019 (also around 40 per cent; Leitner 2021). Moreover, according to the European Training Foundation, health-sector staff (doctors, nurses, midwives, dentists and pharmacists) – and particularly doctors – are the group of professionals the most affected by the Albanian brain drain (ETF 2021).
More than three decades after the first frantic exodus of the early 1990s, when Albanians flocked over the mountainous border with Greece or crowded onto boats bound for Italy (King 2003), the migration is ongoing, only nowadays it is characterised by a departing population which is younger, more educated and professionally qualified (Leitner 2021). Its continuation into the near future seems assured, given recent survey results on ‘potential migration’ – people who declare an intention to migrate. A 2018 survey by King and Gëdeshi (2020) indicated that 29 per cent of survey respondents (N=1,421 for all respondents) expressed their intention to migrate but that the share was much higher – 52 per cent – for the younger cohorts aged 18–40 years; it was 60 per cent for those aged 18–25. Moreover, these figures are higher than those from a similar survey undertaken in 2006, when the population appeared less migration-prone (King and Gëdeshi 2020: 140–141).1
Regarding the poor state of the Albanian health sector, relevant World Health Organization (WHO) and Eurostat data are presented by Mara (2023). In 2020, Albania spent 3.2 per cent of its GDP on publicly funded health, lower than all of its Western Balkan neighbours (for instance, Serbia 5.1 per cent or Bosnia and Herzegovina, 6.4 per cent) and much lower than Germany (8.6 per cent) or the EU average (8.1 per cent). Bear in mind that these percentages are of vastly differing levels of GDP per capita, which depresses the real situation in Albania even further. As a result of a combination of under-investment and emigration, Albania has the lowest density of doctors per 100,000 population in Europe. According to WHO figures quoted by Mara (2023: 36), the ratios for 2020 are as follows: Albania 188, Bosnia and Herzegovina 232, Montenegro 274, North Macedonia 296, Serbia 270, Germany 446 and the EU as a whole 374.2 Finally, gross monthly earnings for health professionals in Albania are, once again, the lowest in Europe – less than one third of the EU average, less than one quarter of the level in Germany and below one fifth of the Swiss figure, based on purchasing power parities (Mara 2023: 39).
Aims, questions and methods
Our broad aims in the paper are threefold.3 First, we aim to document the history and scale of the exodus of doctors, including destination countries and the socio-demographic characteristics of the emigrant doctors. Second, we seek to uncover the causes and consequences of the brain drain of doctors from Albania. Third, looking to the future, we ask: What are the prospects for the ‘diaspora of doctors’ to return to Albania?4 If, however, return was not an option for many individuals, to what extent are the emigrant doctors willing to contribute to and cooperate with their home country in other respects?
Given that, in Albania, the emigration of doctors is a hot topic much discussed in government and other circles, yet with hitherto only anecdotal evidence, we see our paper’s main function as an information-gathering exercise based on robust survey data. Whilst the robustness of our research data is compromised by our inability to claim that it is based on true random sampling, it is enhanced by a sequenced mixed-method approach which starts with a large-N online survey and then continues with a smaller-N round of interviews. We follow the conventional definition of mixed methods as research which ‘collects and analyses data, integrates the findings and draws inferences using both quantitative and qualitative approaches or methods in a single study’ (Tashakkori and Cresswell 2007: 3–4). Provided the two kinds of data collection are carefully aligned and planned in advance to respond to the same set of research questions, ‘triangulation’ – the comparison and confirmation of findings – can improve the validity of the research results (Gamlen 2012: 321).
In order to gather data to respond to the above aims and questions, our research design comprised three stages. First, we carried out a review of literature and statistics from Albanian and international sources, although these yielded only partial insights as the phenomenon of Albanian doctors’ migration is not well-documented. The second stage and principal method was an online survey of Albanian medical doctors who live and work abroad, mainly in Europe. The survey was administered during the period November 2022 to March 2023 and elicited 301 valid responses. The third stage consisted of 25 follow-up qualitative interviews with emigrant doctors who had answered the survey questionnaire and indicated their willingness to take part in an interview. Given the distance factor, most of the interviews took place via zoom but a few were face-to-face when the interviewees were visiting Albania. The interviews were selectively transcribed and translated into English; they provide nuanced insights to complement the survey data.
As there is no register of Albanian doctors working abroad, a major challenge was how to access the survey population. We used various contact strategies: initially a range of respondents who were part of the first author’s personal, social and professional networks. This early approach was followed by social-media networks such as Facebook and LinkedIn; and snowballing out from prior respondents who were asked to recommend friends and colleagues who were also Albanian doctors working abroad.
After establishing an initial contact via email, a copy of the online questionnaire was sent, together with a covering letter outlining the purpose and scope of the survey. Two reminders were sent at monthly intervals to non-respondents. Around 45 per cent of the individuals to whom the survey was sent answered the questionnaire. We feel that this is an acceptable level of response to an online survey of this kind where there is no obligation to respond and no payment for doing so.5
That said, we cannot be categorical about the degree of representativeness of the sample of respondents. We cannot claim an absence of bias between those who responded and those who did not; nor between the sample respondents and those doctors abroad whom we were not able to contact.6 Nevertheless, given the large number of questionnaire respondents (301) and the reasonable number of qualitative interviews (25), we feel that our results are, at least, indicative and, in fact, very revealing.
The online survey consisted of eight blocks of questions:
- basic demographic data of the respondent (age, gender, civil status, country of birth and of current residence);
- education and work experience before emigrating;
- reasons for migration and for choice of destination country;
- studies completed abroad, if any (level, specialisation etc.);
- employment abroad;
- social networks and social capital (both with colleagues abroad and in Albania);
- prospects for returning to Albania (desire to return, when, what kind of job, reasons to return or not to return, conditions for return, obstacles to return etc.); and
- for those not intending to return, cooperation envisaged with Albania (what type of collaboration, obstacles to collaboration etc.).
These questions and subquestions were designed both to yield a comprehensive profile of the phenomenon of Albania’s brain drain of doctors and to shed light on the aims and research questions enunciated earlier.
For the interviews, we chose 25 out of the larger number who consented to be interviewed. This selection was made on the basis of gender balance, country of qualification and country of current residence, with the dual aim of achieving both representativeness and variety across the survey respondents. We found that a high level of ‘saturation’ of interview data – in terms of experiences, perceptions and views expressed – was gained with this number of participants. This number is also consistent with the research literature’s views on ‘How many interviews is enough?’ (Baker and Edwards 2012; Green and Thorogood 2004; Guest, Bunce and Johnson 2006). For instance, Green and Thorogood (2004: 102–104) maintain that, if research is focused on a single participant category (e.g. Albanian doctors working abroad), ‘little new information is likely to be generated after interviewing 20 people’. From the interview transcripts, quotes were strategically chosen to represent consistently expressed views and experiences in shedding light on our research questions.
History, structure, size and characteristics of Albania’s ‘diaspora of doctors’
The first set of questions is addressed via a combination of the methods described above: secondary literature and statistics, questionnaire survey data and qualitative interviews.
Development and typology of the medical diaspora
On the basis of multiple sources, we propose a fourfold typology in the evolution of the emigration of Albanian doctors.
First, there was a large-scale emigration of Albanian doctors during the 1990s, part of a wider-scale brain drain which saw substantial shares of the Albanian scientific and professional elite emigrate abroad during the first, highly chaotic decade of the post-socialist transition (Gëdeshi and Black 2006). During this first phase and also subsequently, many Albanian doctors emigrated to the United States through the Diversity Visa Program for qualified individuals and their families. Some of them were able to get their medical degrees recognised by taking extra exams or following additional specialist training; others, however, ended up working below the level of their skills, experience and qualifications. Based on the 2012 American Community Survey, Nedelkowska and Khaw (2015: 5) estimated that, after 1990, 1,700 first-generation Albanians with degrees in medicine emigrated to the US. Although there is no exact record of the number continuing to work as doctors, a graph in the same report (2015: 7) indicates that just over 1,000 were working in ‘medical science and services’ in 2012. Further insights are offered by Gjergji, one of the US-based interviewees who moved there in the early 1990s:
A small number of [Albanian] medical doctors were integrated, because they arrived here when they were young and took what were called ‘boarding exams’; they obtained high scores and are working as medical doctors… The key to success was to get high scores. Many Albanian doctors who emigrated [to the US] in the 1990s were in their 40s and 50s; they may have been good doctors in Albania but they failed to score high enough in these entry exams. Some of them work in hospitals in other capacities, others shifted to other professions… They are well-paid but they do not make as much as they could [if they had been classified as professional medical doctors].
According to our questionnaire data, about 8 per cent of the Albanian doctors abroad belong to this early-emigrated group who left during the 1990s.
A second group of survey-respondent doctors are Albanian students who, having completed high school in Albania, did their medical degrees abroad and stayed abroad after graduation, either in their study country or another one. Our survey results show that 32 per cent of the respondents pursued the study-abroad route. Italy was the most popular choice for a foreign medical school but many other OECD countries were represented, including Germany and the UK as the next most important.
The third group, accounting for more than half (54 per cent) of the online-survey respondents, is made up of doctors who did their training in Albania and then moved abroad for employment, some immediately after graduation, others after some years working in Albania. Most went to Italy and Germany. The latter country became more attractive after 2016 and the institution of the ‘Western Balkan Regulation’ which proactively facilitated the immigration of already qualified young doctors from Albania and the neighbouring countries of the region (Mara 2023: 35, 39).
The fourth group are the children of Albanian emigrants abroad, either born abroad or taken abroad as children by their migrating parents. The children then pursued their medical studies in their parents’ host country. They account for the smallest fraction of our online survey – 6 per cent – but this could be an under-estimate of their true size since they may be beyond the reach of our survey’s access points.
How many Albanian doctors are there abroad?
An initial issue to be problematised is the definition of the term ‘Albanian doctor’. In the previous subsection, we took a deliberately broad, ethnicity-based approach. A much narrower definition would be to confine the label to those who received their medical training in Albania and subsequently emigrated to work as a doctor abroad: 62 per cent of the online survey sample conform to this stricter definition. A more ambiguous category are high-school-leaver Albanians who take their medical degrees in other countries and continue to work abroad: some would argue that they are not emigré doctors since they did not emigrate as doctors and, hence, constitute less of a medical brain drain. Furthermore, the distinction between the two categories (trained in Albania, trained abroad) is not always clear-cut in cases where, for instance, an individual takes their first medical degree in Albania followed by specialised training or a PhD abroad.
In the absence of a definitive register of doctors who have emigrated from Albania, we can only draw inferences from various sources which are themselves estimates or otherwise debatable. Three main sources can be noted. First, the Albanian Order of Physicians has the function to issue a ‘Certificate of Good Conduct’ to medical doctors who wish to emigrate and practice their profession abroad (Gjypi 2018). In an interview, the President of this Order told us that 809 doctors received the Certificate during the years 2018–2022. As an indication, this represents around 61 per cent of the 1,322 students who graduated from the Medical Faulty of the University of Tirana over the same period. However, not all medical graduates who emigrate necessarily have the Certificate and there are other universities in Albania which run degrees in medicine.
The second source consists of OECD data on ‘foreign-educated’ medical doctors in OECD countries. According to this source, there were 1,161 Albanian doctors working abroad in OECD countries in 2021.7 This source also enables comparisons to be made and Table 1 sets the figures for Albania alongside those for the other Western Balkan countries. Some caveats need to be made about this source. It excludes the (probably small) number of Albanian doctors working in non-OECD countries. More importantly, it excludes Albanian doctors who studied and qualified abroad and then remained abroad. It also excludes, during the last years, those who work in the USA (107 doctors in 2016; no data since then). This means that the data in Table 1 are under-estimates.
Table 1. Emigration of medical doctors from Albania and the Western Balkans
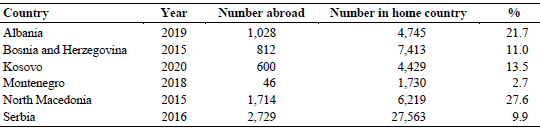
Source: ETF (2022); Mara (2023); OECD (2019).
Finally, there are fragmented data from individual host countries. Those for the USA were noted above. The most significant European country is Germany, which recorded 988 Albanian medical doctors in 2021, a nearly sevenfold increase from 149 in 2013. Other figures which we were able to source were for Switzerland (42 Albanian doctors), the UK (32) and Austria (25). When combined, these statistics indicate that the real size of the Albanian doctors’ diaspora is considerably larger than the OECD figure and, based on the German data, is increasing rapidly.
Our own estimate, based on the various figures quoted above and on email and contact lists sent out for the online survey, is that the diaspora of Albanian doctors lies within the range 2,000–2,500 and possibly higher. This figure equates to around half of the number of doctors working in Albania.
Destination countries
According to answers from the online questionnaire, Albanian doctors are working in 20 countries around the world. In order of importance, these are Germany (35.3 per cent), Italy (23.7 per cent), the US (14.3 per cent) and the UK (9.0 per cent); hence, 82.3 per cent in these four countries. Table 2 shows the remaining countries, down to a threshold of 2 per cent of the total (N=301). Countries with a handful of Albanian doctors but fewer than 2 per cent include Austria, Belgium, Turkey, Sweden, Norway and the Netherlands.
Table 2. Countries where Albanian doctors trained abroad and are working abroad
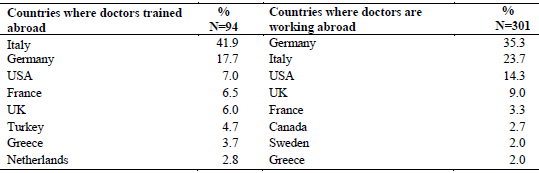
Source: Authors’ survey, 2023.
Interestingly, the countries of current work and residence do not correspond very closely to those where students who did their medical training abroad studied. As Table 2 shows, Italy replaces Germany at the top of the list, Germany is second, followed at some distance by the US, France, the UK, Turkey, Greece and the Netherlands, all above the 2 per cent threshold. Below this threshold for studying medicine abroad we find Switzerland, Austria, Romania, Bulgaria, Sweden, Canada, Portugal and Ireland.
We thus observe that some countries which are geographically near Albania (notably Italy and Greece) or where living costs and tuition fees are low by European standards (Turkey, Romania and Bulgaria) are chosen as logistically and economically convenient places to study but not necessarily to pursue a working career. Having said that, most of those who did their medical training in Italy do continue their medical careers there. However, there is also a tendency for some of those trained in Italy, as well as many of those with degrees from Greece and Turkey, to advance their careers by onward-migrating to more-wealthy countries in Europe and North America, where higher incomes, better career options and more agreeable living conditions are available. The following interview extract from Shpëtim, in Italy, shows how Italy can be used as a launch-pad for a mobile medical career in countries with more advanced and specialised health systems:
In the future, I would like to move to another country, an English-speaking country… Italy, when compared to Albania, has many positive features. However, when compared to other developed countries in Europe, it lags behind in terms of its economy, research and other aspects… I would like to go somewhere where there is a larger international [medical] community… I would feel more at home there.
An important characteristic of the Albanian doctors’ diaspora is its fast growth, especially over the decade since the passing of Germany’s Employment Regulation for the Western Balkans at the end of 2015. The ‘WB Regulation’ was designed to attract doctors from the six countries of the region by recognising their diplomas and offering fast access to vacancies and work and residence permits (Mara 2023). The upward trend is likely to continue in future years, according to the interviewees, in response to Germany’s ongoing shortage of medical doctors.
Interviewees in Germany describe how the country is a ‘perfect combination’ of high salaries and living standards, good working conditions and prospects for professional advancement, generous social security and free education for children. The following extract from the interview with Brunilda, who had recently graduated in medicine in Albania and had just moved to Germany, is typical of those who had moved to this country:
There were 22 students in our graduating class and 17 of them wanted to emigrate, mostly to Germany but also to Italy and Sweden. Germany is the preferred destination because of the simpler procedures to go there… The existence in Tirana of centres offering information about migrating to Germany certainly helps to make the process easier… It is a bit more difficult to go to Italy or Sweden; you need somebody there who can help you, so it takes longer… Italy is attractive as an option because it is close to Albania – which is important for some people – but the salaries there are not as high [as in Germany]. Also, our diplomas are not recognised and so you have to take extra exams… In Sweden, the salaries are high but the language [is a challenge].
Socio-demographics of Albanian emigrant doctors
The first demographic feature that stands out from the online survey is the relatively young age structure of the doctors working abroad. The average age is 37 years and almost three-quarters of them (73.6 per cent) are in the age group 25–40 years. This is in stark contrast to the age profile of doctors in the EU noted earlier – 1 in 3 of whom are aged over 55. From the survey, we find an approximate balance in numbers between men and women, and nearly two-thirds of the respondents (63.7 per cent) are married, some of them to a non-Albanian spouse (which is likely to diminish the likelihood of a return to Albania).
As well as being characterised by their youth compared to the overall population of doctors in Europe and Albania, there are clear indications from our survey respondents, especially the interviewees, that those who migrate are ‘the brightest and the best’. In the view of Dorina, in Germany, the doctors who go abroad are not only high performers in medicine but also high-flyers because they have to learn German (or another language) quickly in order to access and perform their jobs abroad. Gjon, from the US, recounted his experience as follows:
We were 25 students in my class [of medical students]. Of the best students, none are still in Albania… I am in the US, one is in Sweden, most are in Germany. Many of my peers, excellent students of medicine, are no longer in Albania… The elite of Albania’s medical students has emigrated, which I find very sad.
Luan, in Italy, gave a somewhat more variegated diagnosis:
The most ambitious of the medical doctors in Albania emigrate. Those who do not are from medical families who are well-off financially and have their own private practices… Another segment comprises those who did not excel in medical school and lack ambition... Others want to stay close to their families… Lastly, there is a small number who are engaged in politics and, through this, want to climb the career ladder in the healthcare business sector.
Causes and consequences of the emigration of doctors
This is the second cluster of questions addressed by our empirical research, comprising reasons for emigrating, the social and professional experiences accumulated abroad and some reflections on the consequences of this specialised medical brain drain from Albania.
Reasons for emigrating
Survey respondents were presented with a list of 16 possible reasons for emigrating and were asked to select up to 3. From this table we excluded the very small number of respondents who, as ‘second-generation doctors’, declared themselves to have been ‘born in the diaspora’. The reasons were grouped into 5 sets: economic, education, family, health and ‘other’. Table 3 displays the results. The percentage figures refer to all the aggregated factors checked, since each respondent could check a maximum of 3 reasons; hence, for this table, N=542.
Table 3. Reasons for doctors to emigrate from Albania (N=542)
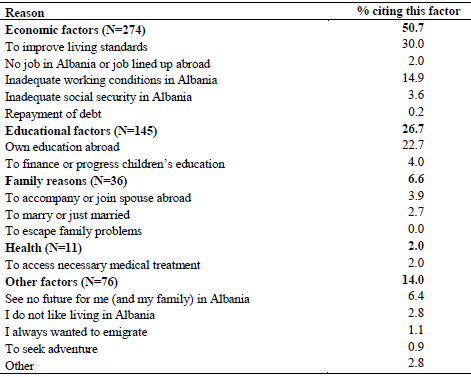
Source: Authors survey, 2023.
Economic factors account for just over half of the aggregated reasons. Although the Europe-wide shortage of doctors constitutes a structural ‘demand-pull’, the economic factors listed in the questionnaire represent a constellation of mainly ‘push’ factors for emigration. The two main elements are the low incomes and poor living standards in Albania (30 per cent) and the poor working conditions (15 per cent). Earlier, we noted that the gross monthly earnings of Albanian health professionals in 2018 were less than one third the EU27 average. In countries like Germany and Switzerland, the salary differential is much greater – 4 to 6 times greater (Mara 2023: 39). Yet, the qualitative interviews reveal that, often, a higher salary is not the main incentive to migrate; rather, poor working conditions and low standards of professionalism in the Albanian health system seem to weigh more heavily. This key point is illustrated from a variety of perspectives in the following interview extracts:
The main factor pushing medical doctors to migrate is [the opportunities for] professional development abroad… specialisation plays a key role. In Germany, when a medical doctor starts his/her job, automatically the specialisation starts… Another aspect is the technology, the equipment available, new research methods and participation in national and international conferences. All these things make our work more interesting and pleasant. So, it’s not only about the salary... but also professional development… The work of a doctor is not just to earn a living; it becomes a mission (Artan, Germany).
Any medical doctor who wants to work [hard], who is passionate about his/her work, who wants to be valued and encouraged to advance and have opportunities for promotion, who wants to lead a normal life… has to go abroad… Certainly most of us would not have left Albania if these things were possible [in our country]. After all, it’s not easy to be an emigrant; you will always be a foreigner in a foreign country (Mirjeta, US).
The second important set of factors scored by the survey respondents are those related to education (27 per cent). This mainly concerns the doctors’ own education and specialisation, including opportunities to do a PhD or join a research laboratory. The quote from Artan, above, speaks to this factor. A small share (4 per cent) underlines the importance of education abroad for their children. Family and health pick up relatively small shares of the reasons checked by respondents – 7 and 2 per cent respectively.
More revealing are some of the factors mentioned under the ‘other reasons’ heading in Table 3, notably the phrase ‘I see no future for me (and my family) in Albania’. There is a general feeling, widespread amongst the Albanian population, especially the younger and more-educated individuals, that emigration is the only way to achieve a ‘normal life’ (see Mirjeta’s quote above) and escape the difficulties, frustrations and disappointments of living in Albania. Quite apart from low incomes and poor career prospects, many interview participants, like Gent in Germany, below, referred to the corruption, the bribery and the need to ‘know the right people’ as endemic features of Albanian society, including the health system.
In Albania, there is always frustration and disappointment. All the time, you see how powerless you are if you don’t know someone [who can help you]… Some of my fellow-students were the children of so-called ‘celebrity doctors’. Upon completion of the specialisation stage, some vacancies suddenly opened up in the University Hospital. All of these new positions were awarded to the children or nephews and nieces of those holding high positions… The rest of us were told that there were no more positions available. Total disappointment, massive corruption. That is the main reason for emigration.
Experiences abroad: professional life, social capital and identity
According to our survey and interview data, Albanian doctors appear to lead socially and professionally satisfying lives abroad yet, at the same time, they maintain frequent contact with relatives and friends in Albania and preserve their Albanian identity. The migrant doctors’ social capital – in the form of formal and informal links to other people, membership of social networks and participation in associations in the host country – is a good indicator of their overall integration. Likewise, social capital linkages back to Albania shed light on our research participants’ material and emotional connections to their homeland, including the possibility of returning there some time in the future.
Two-thirds of survey respondents indicated that they have either ‘frequent’ (31 per cent) or ‘very frequent’ (35 per cent) social contacts with their work colleagues in the host country. This is backed up by interview accounts. Shpëtim’s extract below is a good illustration and also opens up wider insights into the history of Albanian migration to Italy.
I have very good and close relations with my Italian colleagues. We often hang out together after working hours. This is the reality in this city [Milan]. Before, they [Italians] thought that we just came over here [i.e. Albanians migrating to Italy] for a better life. Now they see our migration as a choice we make… Also the image of Albania has changed. Italians visit Albania and see it as a beautiful and fast-developing country.
The latter part of Shpëtim’s quote refers to the enhanced image of Albania and Albanians in the eyes of the Italian population. Back in the 1990s, Albanian immigrants in Italy were stigmatised as rough, uncivilised people prone to criminality (King and Mai 2002). In more recent decades, Albanians have changed that image, largely through their individual efforts of working hard and trying to assimilate into Italian society in an unobtrusive way (King and Mai 2008).
At the same time, Albanian doctors abroad retain strong ties to the home country. According to the responses to the online survey, 96 per cent keep in regular contact with family members in Albania and 69 per cent with friends; however, fewer are in regular touch with colleagues working in the Albanian health sector (38.5 per cent). Communication is maintained via the usual means: phone, email, Skype, WhatsApp, FaceTime etc. Here is a typical statement from Lindita, who has been living in France for 10 years:
I speak to my family every day and I am up-to-date with everything that happens in Albania… I receive information from family and friends who are still in Albania.
Visits to Albania are also frequent. From the survey, 40 per cent visit more than once a year and 44 per cent visit on average once a year. Usually, these visits take place during the summer holidays and/or at New Year, with a much smaller share who visit once in several years (14 per cent) or only on exceptional occasions such as funerals or weddings (2 per cent). The less-frequent visitors are mainly living in distant destinations such as North America or Australia.
Through these contacts, as well as the internet and Albanian TV channels accessed abroad, emigrant doctors are generally well-informed about political, economic and cultural developments and events in Albania. As a result – and also by linking up with other Albanians in their host location – they are able to preserve much of their Albanian identity and sense of national belonging. Afërdita, who has just completed her PhD in medicine in the Netherlands, gave her account as follows:
My mind is that of an Albanian. When I wake up in the morning, I first check the news in Albania and then the Dutch news… When I arrived to start my PhD, I was 23 and felt totally Albanian. Perhaps I will feel increasingly Dutch as the years go by but I believe I will always remain Albanian in my heart.
Compared to the close family and social links that respondents keep with Albania at a personal level, their more organised or ‘structural’ social capital – by which we mean membership of more formalised social networks and associations – is rather weak. According to the online survey, only 18.4 per cent of respondents participate in Albanian associations, organisations or formalised networks in the host countries; mostly these are medical associations, cultural organisations or student bodies. Most of these associations are small, given the limited number of Albanian doctors in most of the countries surveyed.8
Consequences
Undoubtedly, the large scale of the emigration of doctors from Albania has deleterious effects on the country’s health sector and, thus, damages the health and wellbeing of the Albanian population, who are deprived of at least some of the care they need unless they are able to pay for expensive private treatment.
There are regional effects, too. Health services are especially scarce in rural areas and many regional hospitals suffer from the lack of specialist doctors and surgeons. The international emigration of doctors is interwoven with doctors’ internal migration from rural, peripheral areas of the country to the capital, Tirana. Indeed, 57 per cent of medical doctors in Albania are concentrated in the capital city (Gjypi 2018). There is a further knock-on effect in that this is one of the reasons often cited by poor Albanian families who migrate or seek asylum in EU countries in the absence of satisfactory healthcare in the home country (Gëdeshi and King 2022). Likewise, the powerful currents of internal migration, overwhelmingly focused on the Tirana urban region, are partly driven by the lack and poor quality of health services in rural areas and provincial towns (Vullnetari 2012).
Above all, the emigration of doctors and other healthcare professionals inflicts a heavy financial cost on Albania, already a very poor country by European standards. In its study on the Cost of Youth Emigration, the Westminster Foundation for Democracy (2020) estimated that, in 2018, the cost of the upbringing and education of a young emigrant in Albania amounted to 9,267 euros for those with secondary education and 18,283 euros for those having completed tertiary education. The per capita cost of educating emigrating doctors will be even higher, given their long and expensive training. As a result, the country loses millions of euros every year owing to emigration in general and the brain drain of doctors in particular.
The role of the doctors’ diaspora in developing the health system in Albania
The diaspora of Albanian medical doctors has the potential to contribute to the improvement of the home country’s health system in two ways. The first is the return of doctors who have experienced high-quality training, specialisation and medical practice in the health systems of advanced OECD countries. The second is cooperation between the medical diaspora and healthcare institutions, research institutes and university medical schools in Albania. These two development-oriented processes are the final set of issues we address.
What prospects for return?
Economists argue that the return migration of experienced and high-skilled migrants, such as doctors, can generate a positive stimulus to the economic and social development of the countries of origin by introducing new ideas, technologies, skills and experiences and financial capital acquired abroad (Lucas 2005: 244–248; Wahba 2022). Thus, ‘brain return’ compensates for the preceding brain drain.
Unfortunately for the ‘brain return’ hypothesis, only 15 per cent of Albanian doctors working abroad want to return home, according to our survey. More than half, 53 per cent, declare that they do not intend to return while the remainder, 32 per cent, say that they are undecided. Theoretically, the return of doctors with experience, training and specialised knowledge gained from working abroad should boost the standard of medical expertise in Albania. The potential exists for this return transfer of enhanced human capital – so why do only 1 in 7 Albanian doctors working abroad want to return? The reasons are varied and bear a close resemblance to the factors which led to the doctors’ emigration in the first place. They are best articulated by our sample of 25 interviewees.
Synthesising the narratives of the interviewed participants, many say that they have become well-integrated in their respective host countries, having made good economic and career progress which they are sceptical of being able to build on were they to return to Albania. Many doctors have already started a family abroad, some with a non-Albanian spouse. Bringing their children back to Albania and putting them into a different education system, with a switch in the language of instruction, is seen as a formidable challenge – as other studies of ‘returning children’ have shown (Cena, Heim and Triandafiou 2018; Grosa 2022; Vathi, Duci and Dhembo 2016). The doctors also talk about progress in their personal lives which they are unwilling to give up – more disposable income, a better quality of life in a more peaceful and well-ordered environment, new friendship circles and access to cultural and sporting facilities. Others point out that, in spite of some changes and improvements in Albanian living conditions, the medical infrastructure and working conditions are not yet adequate for them to seriously contemplate returning. Finally, interviewees identify corruption, social injustice and insecurity as ongoing problems. Hence, hope for a good future in Albania is largely misplaced. Lindita, interviewed in France, gives a typical account of some of these factors obstructing her return, stressing that salary is not the main factor:
In Albania you don’t need your salary to be as high as in France. I could return for perhaps half of my French salary. However, many other conditions would need to be in place, related not only to the workplace but also to the social aspect… I am used to the fact that, in my current place, social life is much more important… Social and cultural conditions are just as important as work for me. In order for me to return, all these conditions need to be in place. I don’t see that happening in the next 5–10 years. So perhaps I will return only when I retire, buy a house by the sea and enjoy my Albania.
Just under a third of the survey respondents answered that they are undecided whether they will stay abroad or return at some point in the future. Luan (in Italy) is typical of this group:
I have certainly thought about returning. In fact, I think about it all the time. After all, Albania is my country; regardless of the situation there, it is my country. But I don’t know… I have friends who are medical doctors there so I am quite familiar with the health system [in Albania] and I know how problematic it is… At the moment, it seems difficult to become part of that system… Yet, in the future, I would not exclude it [returning].
Both Luan’s and Lindita’s narratives indicate that the return of doctors to Albania is contingent on the existence of some improvements in the country. In the questionnaire survey we asked the ‘undecided’ group about the preconditions which would need to be in place for them to seriously consider return. Respondents were given a list of possible elements and invited to tick as many as they thought relevant to their decision-making. Table 4 presents the results, which are largely self-explanatory. The percentage figures refer to the proportion of the sample answering this question (N=93) who cited each of the preconditions listed.
Table 4. Preconditions for the return of doctors to Albania (N = 93)
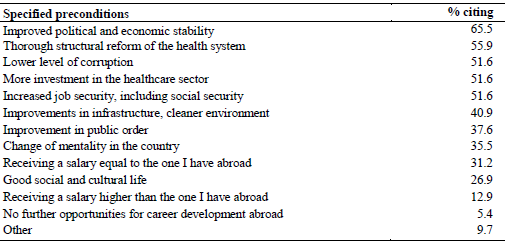
Source: Authors’ survey, 2023.
Cooperation with the diaspora
Given the general lack of desire on the part of Albanian doctors abroad to return home, arguably a more realistic path is to foster the collaboration of the doctors in ways that do not involve them resettling in Albania. Like return migration and development, there is an established and growing literature on diaspora mobilisation as a development-inducing mechanism (see, inter alia, Aguínas 2009; Lucas 2005: 207–229; Sørensen 2007), although little is said in this literature about the specific role of medical professionals in the improvement of the health sector in their countries of origin.
Table 5. Support expressed by Albanian doctors abroad for different kinds of cooperation with the health sector in Albania (N=173)

Source: Authors’ survey, 2023.
According to the online survey, only 11.5 per cent of the doctors abroad have had concrete experiences of collaboration with Albania’s healthcare system. Where cooperation has occurred, it has been sporadic and mainly initiated by the doctors themselves. The forms of collaboration reported include medical consultancies, joint scientific studies and papers, participation in conferences and seminars, guest lectures and media interviews (the last of these especially during the Covid period). Yet, almost 60 per cent of respondents say that they ‘would like to cooperate’ with healthcare institutions and medical research initiatives in Albania. Table 5 sets out the types of cooperation that respondents would like to support – a wide variety of initiatives for joint work. Since respondents could cite multiple forms of cooperation, the percentage scores (as for Table 4) do not sum to 100 but refer to the share of the sample answering this question (N=173) who checked each type of collaboration.
The problem seems to be that reciprocal willingness is not forthcoming from the Albanian side, even though many respondents and interviewees indicate that they would be willing to offer their expertise for zero payment. To illustrate some of the points mentioned above, we quote extensively from the interview with Alban in Switzerland:
We are willing to cooperate but we are not sure whether the same willingness is present in Albania. I visit Albania at least twice a year; I have my father, relatives and friends there. I know colleagues working in cardiology [his specialist field]… but I have not heard of any initiatives being taken.
Alban sees the collaborations as not just one-way – from the ‘expert’ diaspora doctors to the ‘less expert’ doctors in Albania. Rather, he sees the collaboration as
an exchange of experiences from both sides. Perhaps colleagues from Albania could come to our clinics [in Switzerland] and follow a specialised training course… On the other hand… doctors and colleagues here are willing to go and help people in need, who do not have the financial resources [for the treatment they need]. If there are the requisite infrastructures in place in university clinics [in Albania], there are surgeons and cardiologists who could go several times a year for surgeries and to cooperate with colleagues from Albania. I can think of several other positive examples. For instance, an internationally renowned Albanian surgeon in Switzerland regularly visits Prishtina [in Kosovo] and carries out expert surgeries there.
As Alban’s final remark shows, cooperation is not limited to Albania – and both the survey respondents and the interviewees confirmed their willingness to collaborate with Kosovo, which is predominantly ethnic-Albanian, and North Macedonia, where there is a large minority of ethnic Albanians.
Conclusions and policy suggestions
Over the past decade, Albania has experienced a rapid increase in the emigration of medical doctors, recording one of the highest rates in Europe. This trend looks likely to continue, unless remedial measures are taken. Those who leave are distinguished by their youth and ambition. The emigration of Albanian doctors represents a massive loss of both human capital and investment in the production of that human capital – a significant part of the 559 million euros annually that the Westminster Foundation for Democracy (2020) estimates is lost to the country through the emigration of its young people. For the doctors in our survey, the financial loss of their training is greater for those fully trained in Albania prior to emigration than for those who are educated in Albania up to high school and then do their medical degrees abroad.
It is true that the cost of the medical brain drain could be reduced if medical studies were not so highly subsidised from the public purse and students had to bear a higher share of the costs by paying higher fees or taking out loans. Theoretically, such a measure would partially solve the financial impact of the brain drain but, at the same time, this would be self-defeating since most students, except those from very wealthy families, would never be able to afford to study medicine.
Most Albanian emigrant doctors do not intend to return to Albania. This is arguably our key finding and the most worrying one for the future of the Albanian healthcare sector. Here we come back to a fundamental dilemma intrinsic to the debate on brain drain noted earlier. How can we reconcile the individual’s right to migrate in order to achieve self-improvement with the structural inequalities and injustices in the global supply and demand for medical professionals? Most of the interviewees are acutely aware of this tension at the heart of their behaviour. They gave powerful justifications for their decision to leave Albania yet, at the same time, expressed unease and sadness that the best of Albania’s young doctors are lost to the country.
The obstacles to return are more or less the same factors that drive the emigration. Low salaries in Albania are, of course, important but equally, if not more so, are working conditions, prospects for career development and the overall social and political environment in Albania. If there is one phrase that encapsulates both the decision to leave and the reluctance to return, it is that ‘there is no future in Albania’. These factors are not unique to doctors but have been found to be equally relevant in surveys we have carried out on the Albanian population as a whole (King and Gëdeshi 2020) and of specific segments of the population such as the ‘scientific diaspora’ of PhD-holders (Gëdeshi and King 2021) and university students (King and Gëdeshi 2023).
Moving from the ‘knowledge production’ of our key findings summarised above to ‘knowledge utilisation’ leads us into what has been called the ‘research–policy nexus’ in migration studies (Scholten 2018). We identify three fundamental policy questions. How can the emigration of young doctors be staunched? How can those abroad be encouraged to return? Finally, given that many doctors will not return, how can the ‘diaspora of doctors’ be mobilised to help develop the Albanian health system in other ways? Many helpful insights are given by the survey respondents and interviewees. Here, we summarise and put structure to these suggestions and answers.
First and foremost, the Albanian health system needs major reform and increased resourcing so that doctors are offered not just a satisfactory income but also, more importantly, good working conditions and continuous professional advancement in an environment that is secure and better-equipped. Albania should aim at EU levels of investment in its health services in terms of the share of GDP – at least 8 per cent, a more than doubling of its present share. How to boost this spending level raises the old question of ‘taxing the brain drain’ (Bhagwati 1976). A tax on immigrant earnings in more-developed countries to compensate for the highly skilled emigrants’ education in their less-developed countries of origin could be considered as an act of international redistributive justice. Such a proposal is administratively challenging and can fall prey to tax evasion. Furthermore, there is the task of ensuring that such repatriated tax revenue is productively used to improve Albania’s health training and delivery systems.
Second, one way to boost the supply of doctors would be to increase the number of medical students by expanding quotas and opening up new faculties of medicine. Cooperation could be sought from established medical schools in Europe to advise on curriculum planning and resources, supported by staff and student exchanges and internships. The obvious danger of this policy – that the extra supply of doctors would only lead to more brain drain – would need to be countered by other policies. One of these relates to a new law approved by the Albanian parliament in September 2024 which requires medical graduates trained in Albania to remain in the country for at least 3 years. However, the likely outcome of this regulation will be to push more Albanian medical students to pursue their studies abroad.
Third, both within the medical sector and in the broader realm of Albanian society and governance, there needs to be created a more transparent, meritocratic ethos, free of corruption, nepotism and a culture of bribery and favours. The health system should be immune to political influence or the interference of other power brokers.
Fourth, given the evidence presented in the online survey and the interviews that the current diaspora of doctors abroad has a low likelihood of returning but is more open to various forms of collaboration, plans should be put in place to manage cooperative efforts, including joint projects and research, training visits and exchanges, lectures and consultancies. Such cooperation can be supported by new and advanced technologies of online communication. Within this framework of diaspora mobilisation, there should be a strategy of replacing long-term emigration by circular mobility. This would boost the skills and qualifications of Albanian doctors and bring new ideas and operating systems into the Albanian health sector.
Finally, it would be useful to establish a database of Albanian doctors abroad in order to facilitate cooperation and to attract the return, on a short or longer term, of expertise in needed specialised fields.
Notes
- These survey results are consistent with findings from the Regional Cooperation Council’s annual Balkan Barometer reports. According to the 2023 Barometer survey, 44 per cent of the surveyed population of the 6 countries of the Western Balkans ‘would consider living and working abroad’, as would 71 per cent of youth aged 18–24. For the aggregate population surveyed, the figure for Albania (49 per cent) is significantly higher than the regional average. These figures indicate ongoing increases in intentions to migrate since King and Gëdeshi’s 2018 survey (2020), although attention should be paid to the wording of the key question, which can influence response rates.
- We think that the Albanian figure of 188 might be artificially inflated, since previous years’ figures were consistently lower – in the 120s – and there was no marked increase in the training of doctors in medical schools nor increased investment in the health sector to warrant a jump to 188 in 2020.
- This paper is based on and reproduces some sections from an informally published working paper (see Gëdeshi, King and Ceka 2023).
- We use the term ‘diaspora’ in its descriptive sense of meaning a ‘scattering’ rather than alluding to its historical origin as a process born out of trauma and exile.
- The survey was administered from Albania where there is no formal procedure for ethical approval for this kind of research. Nevertheless, for both the online survey and the follow-up interviews, we adhered to standard ethical procedures of the anonymity of participants and their right to withdraw at any time and general principles of ‘no harm’ to anyone involved.
- Possible sources of bias between respondents and non-respondents include differences in age, gender, specialisation, country of qualification and country of residence and work.
- Data from http://data-explorer.oecd.org/.
- Some of the associations are larger and their membership extends to ethnic Albanians from other Western Balkan countries. As an example, the League of Albanian Doctors in Switzerland has around 400 members from Albania, Kosovo, North Macedonia and Montenegro (see https://www.swissalbned.ch/). The goal of the association is to help Albanian doctors’ integration in the host country, to exchange medical information and expertise through conferences, workshops and online platforms and to collaborate with the healthcare sectors in the doctors’ home countries.
Funding
The authors received no funding for this study, which was carried out in their own research time.
Conflict of interest statement
No conflict of interest was reported by the authors.
ORCID ID
Russell King  https://orcid.org/0000-0001-6662-3305
https://orcid.org/0000-0001-6662-3305
References
Adovor E., Czaika M., Docquier F., Moullan Y. (2020). Medical Brain Drain: How Many, Where and Why? Journal of Health Economics 76, 102409.
Agunías D.R. (ed.) (2009). Closing the Distance: How Governments Strengthen Ties with their Diaspora. Washington DC: Migration Policy Institute.
Baker S.E., Edwards R. (2012). How Many Qualitative Interviews is Enough? Southampton: ESRC National Centre for Research Methods Review Paper.
Bhagwati J.N. (1976). Taxing the Brain Drain. Challenge 19(3): 34–38.
Buchan J., Campbell J., Dhillon I., Charlesworth A. (2019). Labour Market Change and the International Mobility of Health Workers. London: Health Foundation Working Paper 5.
Cena E., Heim D., Triandafiou R. (2018). Changing Places: Children of Return Migrants in Albania and their Quest to Belong. Journal of Ethnic and Migration Studies 44(7): 1156–1176.
Commander S., Kangasniemi M., Winters L.A. (2004). Is the Medical Brain Drain Beneficial? Evidence from Overseas Doctors in the UK. London: Centre for Economic Performance, Discussion Paper 618.
D’Aiglepierre R., David A., Levionnois C., Spielvogel G., Tuccio M., Vickstrom E. (2020). A Global Profile of Emigrants to OECD Countries: Younger and More Skilled Migrants from More Diverse Countries. Paris: OECD, Social, Employment and Migration Working Paper 239.
Docquier F., Rapoport H. (2012). Globalisation, Brain Drain and Development. Journal of Economic Literature 50(3): 681–730.
ETF (2021). How Migration, Human Capital and the Labour Market Interact in Albania. Turin: European Training Foundation.
ETF (2022). Use It or Lose It! How Do Migration, Human Capital and the Labour Market Interact in the Western Balkans? Turin: European Training Foundation.
Gamlen A. (2012). Mixed Methods in Research on Diaspora Policies, in: C. Vargas-Silva (ed.) Handbook of Research Methods on Migration, pp. 319–341. Cheltenham: Edward Elgar.
Gëdeshi I., Black R. (2006). From Brain Drain to Brain Gain: Mobilising Albania’s Skilled Diaspora. Tirana: UNDP.
Gëdeshi I., King R. (2021). The Albanian Scientific Diaspora: Can the Brain Drain Be Reversed? Migration and Development 10(1): 19–41.
Gëdeshi I., King R. (2022). Albanian Returned Asylum-Seekers: Failures, Successes and What Can Be Achieved in a Short Time. Journal of Balkan and Near Eastern Studies 24(3): 479–502.
Gëdeshi I., King R., Ceka A. (2023). Emigration of Medical Doctors from Albania: A Segmented Brain Drain. Brighton: University of Sussex, Sussex Centre for Migration Research Working Paper 101.
Gjypi S.A. (2018). Largimi I Mjerkëve nga Shqipëria (Outflows of Doctors from Albania). Tirana: Friedrich-Ebert-Stuiftung.
Glinos I. (2015). Health Professional Mobility in the European Union: Exploring the Equity and Efficiency of Free Movement. Health Policy 119(12): 1529–1536.
Green J., Thorogood N. (2004). Qualitative Methods for Health Research. Thousand Oaks CA: Sage.
Grignon M., Owusu Y., Sweetman A. (2013). The International Migration of Health Professionals, in: A.F. Constant, K.F. Zimmermann (eds) International Handbook on the Economics of Migration, pp. 75–97. Cheltenham: Edward Elgar.
Grosa D. (2022). The Return Migration of Children: (Re)Integration Is Not Always Plain Sailing, in: R. King, K. Kuschminder (eds) Handbook of Return Migration, pp. 241–254. Cheltenham: Edward Elgar.
Guest G., Bunce A., Johnson L. (2006). How Many Interviews Are Enough? An Experiment with Data Saturation and Variability. Field Methods 18(1): 31–44.
INSTAT (2024). Albania Population and Housing Census 2023. Tirana: INSTAT.
King R. (2003). Across the Sea and Over the Mountains: Documenting Albanian Migration. Scottish Geographical Journal 119(3): 283–309.
King R. (2018). Is Migration a Form of Development Aid Given by Poor to Rich Countries? Journal of Intercultural Studies 39(2): 114–128.
King R., Mai N. (2002). Of Myths and Mirrors: Interpretations of Albanian Migration. Studi Emigrazione 39(145): 161–199.
King R., Mai N. (2008). Out of Albania: From Crisis Migration to Social Inclusion in Italy. New York: Berghahn.
King R., Gëdeshi I. (2020). New Trends in Potential Migration from Albania. Migration and Development 9(2): 131–151.
King R., Gëdeshi, I. (2023). Albanian Students Abroad: A Potential Brain Drain? Central and Eastern European Migration Review 12(2): 73–97.
Kroezen M., Dussault G., Craveiro I., Dieleman M., Jansen C., Buchan J., Barriball L., Rafferty A.M., Bremner J., Sermeus W. (2015). Recruitment and Retention of Health Professionals Across Europe: A Literature Review and Multiple Case Study Research. Health Policy 119(12): 1517–1528.
Leitner S. (2021). Net Migration and its Skill Composition in the Western Balkan Countries between 2011 and 2019: Results from a Cohort Approach. Vienna: Vienna Institute for International Economics, wiiw Working Paper 197.
Lucas R.E.B. (2005). International Migration and Economic Development: Lessons from Low-Income Countries. Cheltenham: Edward Elgar.
Mara I. (2020). Health Professionals Wanted: Chain Mobility across European Countries. Vienna: Vienna Institute for International Economic Studies, wiiw Research Report 445.
Mara I. (2023). Health Professionals Wanted: The Case of Health Professionals from Western Balkan Countries to Europe. Central and Eastern European Migration Review 12(2): 33–52.
Nedelkowska L., Khaw N. (2015). The Albanian Community in the United States: Statistical Profiling of the Albanian-Americans. Cambridge MA: Harvard University, Center for International Development.
OECD (2019). Recent Trends in International Migration of Doctors, Nurses and Medical Students. Paris: OECD Publishing.
Scholten P. (2018). Research–Policy Relations and Migration Studies, in R. Zapata-Barrero, E. Yalaz (eds) Qualitative Research in European Migration Studies, pp. 287–302. Cham: Springer.
Sørensen N.N. (ed.) (2007). Living Across Worlds: Diaspora, Development and Transnational Engagement. Geneva: International Organization for Migration.
Tajdens F., Weilandt C., Eckert J. (2012). Mobility of Health Professionals: Health Systems, Work Conditions, Patterns of Health Workers’ Mobility and Implications for Policy Makers. Berlin and Heidelberg: Springer.
Tashakkori A., Cresswell J.W. (2007). The New Era of Mixed Methods. Journal of Mixed Methods Research 1(1): 3–7.
Vathi Z., Duci V., Dhembo E. (2016). Homeland Dis(Integrations): Educational Experience, Children and Return Migration to Albania. International Migration 54(3): 159–172.
Vullnetari J. (2012). Albania on the Move: Links between Internal and International Migration. Amsterdam: Amsterdam University Press.
Wahba J. (2022). The Economics of Return Migration, in: R. King, K. Kuschminder (eds) Handbook of Return Migration, pp. 24–37. Cheltenham: Edward Elgar.
Westminster Foundation for Democracy (2020). Cost of Youth Emigration: Albania. London: UK Foreign, Commonwealth and Development Office.
Wismar M., Maier C.B., Glinos I.A., Bremner J., Dussault G., Figueras J. (2011). Health Professional Mobility and Health Systems in Europe. Brussels: European Observatory on Health Systems and Policies.
World Bank (2016). Migration and Remittances Factbook. Washington DC: The World Bank.
Copyright information
© The Author(s)
Open Access
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.