Health Professionals Wanted: The Case of Health Professionals from Western Balkan Countries to Europe
-
Author(s):Mara, IsildaPublished in:Central and Eastern European Migration Review, Vol. 12, No. 2, 2023, pp. 33-52DOI: 10.54667/ceemr.2023.24Received:
26 August 2022
Accepted:1 December 2023
Published:7 December 2023
Views: 3924
The Western Balkan countries have been faced with a rising outward mobility of health professionals, driven by the increasing demand for this category of worker, especially in European countries. Labour-market imbalances are pushing many health professionals to leave the Western Balkan region. As a consequence, shortages of health professionals are looming and access to health services in the region is put under strain. The purpose of this study is to shed light on the recent pattern of mobility of health professionals from Western Balkan (WB) countries. A gravity model is implemented to analyse the push-and-pull factors of mobility during 2000–2019 and towards European countries. The analysis finds that income differentials between WB and European countries are strong pull factors. Additionally, policy changes in the destination countries shape the mobility patterns and several European countries, especially Germany, have benefited from the mobility of health professionals from WB countries.
Introduction and background information
The literature about the migration of health professionals, the drivers of this kind of mobility and its effects on the sending and receiving countries has been expanding rapidly. This has been motivated by the fact that many countries in the world are facing a rising demand for health professionals which cannot be tackled simply with health professionals trained at home. By 2030, the global demand for health professionals will double with respect to the previous decade but the supply of this category of workers will not be changing at a similar pace. Therefore, shortages of health professionals will prevail (see Liu, Goryakin, Maeda, Bruckner and Scheffler 2017; Scheffler, Campbell, Cometto, Maeda, Liu, Bruckner, Arnold and Evans 2018). In this context, foreign-trained health professionals have played and are expected to continue to play an important role (Grignon, Owusu and Sweetman 2013; Mullan 2005; OECD 2015). This issue became even more evident during the Covid-19 pandemic (Scarpetta, Dumont and Socha-Dietrich 2020).
At an international level, several studies have revealed that the drivers of health professionls’ mobility can be both supply- and demand-driven (Buchan, Campbell, Dhillon and Charlesworth 2019; Davda, Gallagher and Radford 2018; Kroezen, Dussault, Craveiro, Dieleman, Jansen, Buchan, Barriball, Rafferty, Bremner and Sermeus 2015; Maeda and Socha-Dietrich 2021; Tjadens Weilandt and Eckert 2012). On the demand side, the retirement of baby-boomers, the rise in life expectancy and the ageing of the population are generating an ever-greater need for health professionals. On the supply side, better working conditions and earning opportunities abroad have been a magnet for many health professionals, especially those from the less-developed or developing countries. Some of the key findings of the studies cited above are that the receiving countries – mainly developed countries – have been benefiting from the mobility of health professionals trained abroad. The effects on the sending countries have been mixed – with both positive and negative effects. The positive effects are more obvious at the micro level, given that health professionals who migrated abroad have been benefiting from a better working environment, skills enhancement and higher earnings in the receiving countries. However, at the macro level, the emigration of health professionals has been accompanied by brain drain, rising shortages of health professionals and a loss of investment in the training of health professionals (OECD 2019b).
The literature indicates that European countries are facing similar challenges as at the global level. Employment in the health sector in Europe has experienced its strongest growth over the past two decades. Yet, because a large share of health professionals are going to retire in the not-too-distant future, demand for new ones will expand (CEDEFOP 2018). Accordingly, many countries in this and the next decade are likely to be characterised by increasing job opportunities in the health sector. Despite the rising number of health professionals in per capita terms, imbalances in the supply and demand of health professionals are prevailing among the European countries. Such imbalances have been generating a continuous battle to attract health professionals and a few wealthier European countries have been benefiting at the expense of poorer ones (Glinos 2015; Mara 2019). The EU15 countries have seen a high degree of outward mobility of doctors – mainly to EFTA countries, the US and Canada. Meanwhile, many doctors who left have been replaced by doctors from Central and Eastern European (CEE) and WB countries.1 Switzerland and Norway have greatly benefited from receiving doctors from the EU15, while sending hardly any abroad themselves. In contrast, CEE and WB countries have experienced an intensive outflow of medical doctors who have barely been replaced by doctors from other countries (Kroezen et al. 2015; Mara 2020; Ognyanova, Maier, Wismar, Girasek and Busse 2012; Schultz and Rijks 2014; Williams, Jacob, Rakovac, Scotter and Wismar 2020; Wismar, Maier, Glinos, Bremner, Dussault and Figueras 2011). Thus, the chain mobility of health professionals has been striking, especially for Eastern European and WB countries. Some of the lessons learned are that further efforts must be made for a better coordination of mobility that would smooth out some of the imbalances stemming from the free mobility of health professionals and reassuring that there are certain mutual benefits both for the sending and receiving countries.
In this context the issue of health professional mobility from WB countries, especially towards European countries, has gained momentum. More than 80 per cent of emigrants from the WB countries reside in one of the European countries, including health professionals (World Bank and wiiw 2018). The free visa regime applied in the Schengen area with respect to citizens from the Western Balkans and also other regulations introduced with respect to high-skilled professionals originating outside Europe (which affect citizens of the Western Balkan countries) – and particularly the Western Balkan Regulation (§26.2 German Employment Regulation) introduced in Germany in 2016 – have reshuffled the mobility patterns of health professionals from the region towards the EU.2
As the international literature suggests, the phenomenon of health professionals’ mobility is very complex and its drivers are related to economic and institutional factors; however, it is also driven by linguistic, cultural and geographical proximity (Adovor, Czaika, Docquier and Moullan 2020). The phenomenon can be accompanied by imbalances in the supply and demand of health professionals, a sectoral-specific brain drain and a loss of investment in their training (OECD 2019b). As such, the health systems in these countries – which already suffer from low investment – end up being part of a vicious circle because investing further in the health system and education of health professionals is perceived as counterproductive. This has further negative repercussions on the accessibility and quality of health services.
Accordingly, the purpose of this study3 is to shed light on recent shifts in the demand and supply of health professionals and the challenges which lie ahead, especially as concerns the WB countries as a sending region and Europe as the main destination region.4 In particular, the aim is to investigate the drivers of mobility of health professionals from the WB and identify the main push-and-pull factors accounting also for policy changes – such as the Western Balkan Regulation (§26.2 German Employment Regulation) mentioned above (Brücker, Falkenhain, Fendel, Promberger, Raab, Trübswetter, Blažević and Trmkoli 2020).
The paper is structured as follows. The next section, following this introduction, presents a broad overview of how the pattern of demand and supply for health professionals has been shifting over the past decade between European countries and also between WB and European countries. The subsequent section analyses the drivers of mobility by using a gravity model that allows for both push and pull factors of mobility at a pair-country level. The following section then presents the estimation results of the gravity model, first starting with a general model of push and pull factors – namely between European and Western Balkan countries – and secondly focusing on the special case of the WB countries. The last section concludes and discusses some policy implications targeting medical doctors’ mobility from WB countries.
Health workforce mobility: stylised facts
Supply and demand of health professionals
The density of the health workforce has improved across all European and WB countries. In 2010 there were 34 medical doctors and 80 nurses and midwives for 10,000 inhabitants whereas, by 2020, these ratios had risen to 43 and 95, respectively (see Figures 1 and 2).
Nevertheless, as the graphs portray, substantial differences prevail with respect to the density of the health professionals across European and WB countries. For a group of European countries (e.g. Sweden, Austria, Germany, Belgium and Finland) the supply of health professionals tends to be above or close to the EU28 average and this has improved further over time – both for medical doctors and nurses and midwives. In contrast, the WB countries are at the bottom of the ranking for the number of health professionals in per capita terms and their levels are far below the EU28 average.
Figure 1. Medical doctors per 10,000 inhabitants, 2010 and 2020
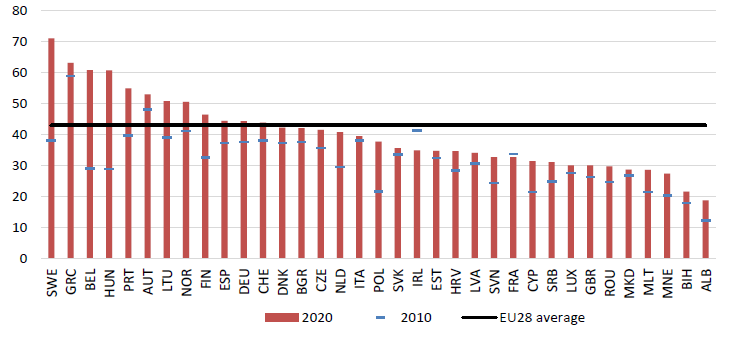
Source: World Health Organisation.
Note: 2020 or the latest year available has been used for a number of countries.
Figure 2. Health professionals: nurses and midwifery personnel per 10,000 inhabitants, 2010– 2020
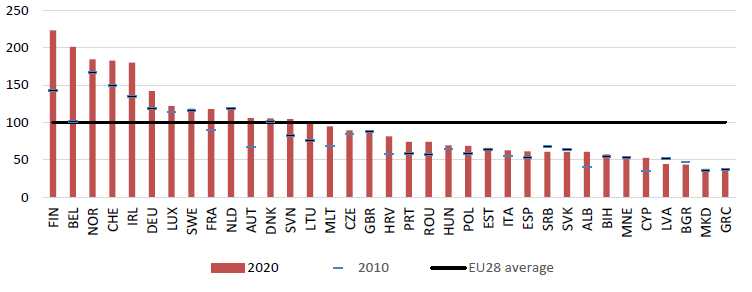
Source: World Health Organisation.
Note: 2020 or the latest year available has been used for a number of countries.
Despite improvements on the supply side, this will not be sufficient to meet needs from the demand side. The pressure on health services and care is expected to increase in the coming decades. Rising longevity and population ageing are putting a strain on healthcare provision. Recent demographic changes suggest that several European countries are experiencing a rise in the life expectancy of their populations (Mara 2020; WHO 2022; Williams et al. 2020). Western Balkan countries are also already showing clear signs of rapid ageing, especially Bosnia and Herzegovina and Serbia (see Figure 3). Such dynamics suggest that not only European but also WB countries will all be facing a rising demand for healthcare – especially for care-based related services – owing to the increasing longevity of their populations.
Figure 3. Population over 65 years by country groups, current and projected trend, in % of total population
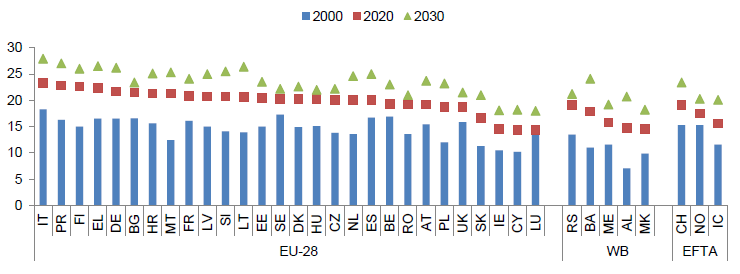
Source: UN Population statistics.
Despite the increase in the supply of health professionals, the rise in demand is such that imbalances and shortages of this category of workers have emerged in a number of European and WB countries (European Commission 2017). Half of the European countries report shortages of medical doctors; this group comprises, in particular, the Nordic countries, the UK, Ireland, Belgium, Germany and the Netherlands, even though these countries have a density of health professionals above the EU28 average. In the EU-CEE countries, medical doctors are in short supply, especially in the Baltics, Slovakia, Slovenia, Croatia and Bulgaria (ETF 2022).
Apart from being demand-driven, shortages in the health workforce are also supply-driven. Quite a large proportion of health professionals in European countries are approaching retirement age. In most countries the share of health professionals above the age of 55 has been rising (Mara 2020) – on average, 1 in 3 health professionals in the EU is over 55. Accordingly, the vast majority of job opportunities for health professionals over this decade will be driven by replacement demand (Mara 2020).
Health professionals’ mobility and push and pull factors
Countries pursue different strategies and policies to satisfy their current and future demand for health workers. In general terms, the demand for health professionals is met through the existing workforce in the health sector, graduates who have qualified in health and welfare disciplines, health professionals who are foreign-born and, more recently, automated technology that is assisting or replacing – to some extent – humans in healthcare.
Satisfying the demand for health professionals with a workforce from abroad has intensified in several European countries. The international mobility of health professionals has been advantageous for a number of net-receiving European countries. However, for the other countries – which are net senders – it has been detrimental and has accentuated further shortages of health professionals. Across Europe, 1 in 10 is foreign-born, with substantial differences noticeable in individual countries. In Ireland, almost half of the medical doctors are foreign-born while, in Sweden, 1 in 3 doctors originates from abroad (Mara 2020).
For some European countries, the turnover of health professionals’ mobility is high. For example, Germany experiences a high exchange of medical doctors. Still, the net effect is negative, suggesting that Germany is a country that is losing medical doctors. In contrast, the number of foreign nurses who move to Germany is twice as high as the number of those who leave. Austria is another country where the outflow of medical doctors is exceeding the inflow whereas, for nurses, the net flow is positive. Other countries, such as Italy and the Netherlands, are losing both medical doctors and nurses. Among Central and Eastern European countries, the net flow of medical doctors and nurses is predominantly negative (Mara 2020). As shown above, the density of health professionals in the WBs is among the lowest in Europe. Despite this, the outward mobility of health professionals has accelerated to unprecedented levels. According to the OECD (2019a) database, the stock of medical doctors abroad from the region was estimated at around 7,000 in 2021. This would correspond to 13 per cent of medical doctors available in the region (Table 1). As far as nurses are concerned, only a partial picture can be obtained about their outward mobility because a number of OECD countries report missing information. As such, the lack of sufficient and accurate data do not allow any sound inference to be made at an aggregate level.
Table 1. Health professionals’ mobility from the Western Balkans: the case of medical doctors and nurses
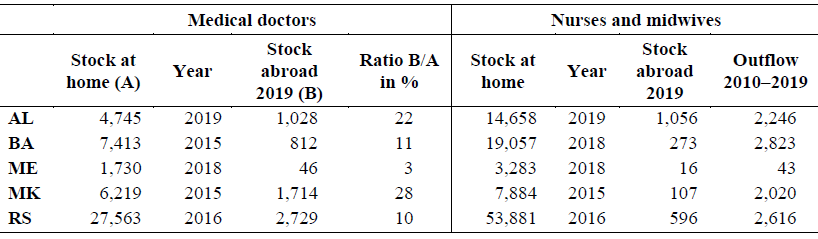
Source: Own elaboration using World Health Organisation statistics for the stock of medical doctors, nurses and midwives at home for Western Balkan countries. OECD (2019a) data are used for the stock of medical doctors and nurses abroad.
As the literature has suggested (e.g. Adovor et al. 2020), a strong pull factor for health professionals is the wage gap between earnings at home and earnings abroad. The comparison across countries of the level of earnings – in euros at purchasing power standards (PPS) – among health professionals, hospital nurses and health specialists shows that there are big gaps, especially between the WB and European countries (Figure 4). As such, the wage gaps are important drivers of emigration, especially for health personnel in the WBs.
In addition, a strong set of push factors for moving abroad are the poor working conditions and lack of employment opportunities in the home country. Public spending on health continues to be low. According to the World Bank, in 2018 the share of health expenditure to GDP in Albania was 5.3 per cent, in Bosnia and Herzegovina 8.9, in Montenegro 8.4, in North Macedonia 6.6 and, in Serbia 8.5; in comparison, in Germany it was 11.4, in Austria 10 and in the EU overall 10 per cent. The private health system is small and in many instances functions as a second source of employment for those already working in the public sector. Country studies unanimously and unambiguously report that health professionals are leaving not only because of better earnings prospects but also because of the poor quality of working conditions and the limited job openings in the WB (see ETF 2022). Rural areas in particular suffer from a lack of health services, due to limited investments in infrastructure, a dearth of medical centres and a consequent shortage of medical staff.
Figure 4. Gross monthly earnings for professionals and associate professionals providing human health and social work services in euros (PPS), 2018
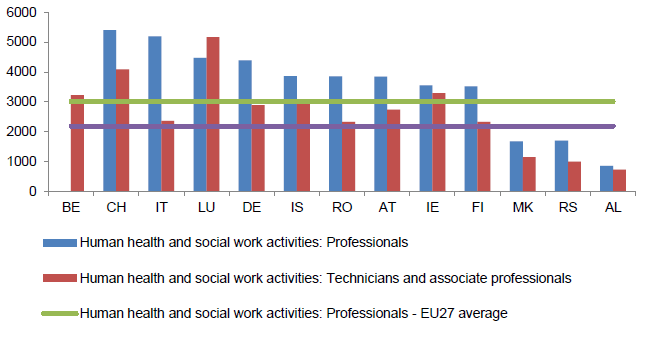
Source: Eurostat: mean monthly earnings by economic activity and occupation [earn_ses18_48].
Policy changes in destination: the case of Germany
Especially over the last 5 years, Germany has turned into an attractive destination for health professionals from the region. As already mentioned, the large income gap between the WB and Germany acts as a strong magnet for low-paid health workers in the region. Nevertheless, another important driver of mobility is Germany’s proactive recruitment policies for health professionals from the WB region, especially the aforementioned Western Balkan Regulation (§26.2 German Employment Regulation). As a result, between 2015 and 2020, the stock of health workers – including doctors, nurses as well as other specialist health professionals such as dentists, pharmacists or physiotherapists – in Germany from the WB6 (Albania, Bosnia and Herzegovina, the former Yugoslav Republic of Macedonia, Kosovo, Montenegro and Serbia) has increased significantly (Figures 5 and 6) based on the data provided by the German Federal Labour Agency. Over this period, Germany has attracted more than 18,000 health professionals from the WBs – representing close to 20 per cent of foreign trained health professionals moving to Germany over the last 5 years. As such the stock of health professionals from the WBs in Germany exceeded 30,000 by 2020 – 2.5 times higher than in 2015 (Schmitz-Pranghe Oruč, Mielke and Ibričević 2020).
More than 37 per cent of health professionals from the WB6 in Germany are from Bosnia and Herzegovina, 28 per cent from Serbia, another 13 per cent each from Albania and Kosovo, 7 per cent from North Macedonia and fewer than 2 per cent from Montenegro. Bosnia and Herzegovina and Serbia continue to be the main sending countries from the WBs to Germany. Albania has recently recorded a strong outflow of health professionals to Germany – between 2015 and 2020 its stock of health professionals there more than quadrupled, rising to close to 4,000. More than 16 per cent of health workers from the WB6 in Germany are ‘health professionals’, mainly represented by medical doctors (more than 70 per cent). The rest consists of associate health professionals, of whom the vast majority are nurses. Besides Germany, countries such as Slovenia, Austria, Switzerland, Croatia, Denmark and Italy, which are in need of health professionals from abroad, have been important destinations for those from the WB region. Beyond the WBs, Germany is an attractive country for health professionals from the EU-CEE, especially for doctors from Romania, Hungary, Bulgaria, Poland and the Czech Republic. Medical doctors from the 2 group of countries – EU-CEE and WB – moving to Germany accounted for close to 60 per cent of the total inflow of foreign-trained doctors to Germany between 2010 and 2018. As for nurses, apart from the EU-CEE countries, recently a large number of them have been coming from Croatia or WB countries, especially Bosnia and Herzegovina, Serbia and Albania.
Figure 5. Health professionals and associate health professionals from the WB6 in Germany and change in the stock of health professionals, 2015–2020

Source: https://statistik.arbeitsagentur.de.
Figure 6. The stock of medical doctors from the WB6 in Germany, 2015–2020 (March)
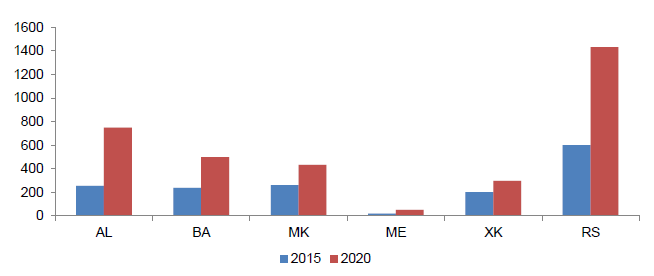
Source: https://statistik.arbeitsagentur.de.
Germany itself is an EU country which has recorded losses of medical doctors, despite receiving many health professionals from abroad. At a numerical level, the inflow of doctors has compensated for 90 per cent of Germany’s outward mobility. As far as nurses are concerned, the inflow has been higher than the outflow. Between 2010 and 2018, more than 14,000 German doctors and 10,000 nurses preferred to leave the country, mainly moving to Switzerland but also to Austria or countries outside the EU. Such outward mobility has been driven by a high demand in these host countries as well as the relatively high wages offered to health professionals in Switzerland, Austria and Luxembourg.
The WB regulation did not impose any restrictions on minimum language or professional qualification requirements. Under the new regulations, there were two main conditions which WB6 citizens had to fulfil to attain a work permit in Germany: first, have a job offer by an employer in Germany (including the ‘priority check’). Second, the job offer should comply with German labour laws and minimum wage standards and should have been approved by the Federal Employment Agency. In late 2020, the German Federal Council (Bundesrat) approved the extension and amendment of the Regulation until 31 December 2023, with a new maximum number of 25,000 permits to be issued per year by the Employment Agency. The new regulation became effective from 1 January 2021.
Migration from the WB6 to Germany has increased enormously thanks to these new regulations, with an increase of 66 per cent between 2010 and 2019 – close to 900,000 people (ETF 2022). Thanks to this regulation, migration from the WBs to Germany rose significantly for health professionals and, in 2020, the health sector was one of these migrants’ top 10 occupations. An important share of them are health associate professionals, which includes mainly medical and pharmaceutical technicians, nursing and midwifery associate professionals and traditional and complementary medicine associate professionals.
Drivers of the mobility of health professionals: a gravity approach analysis
The gravity model of medical doctors’ mobility
For the analysis of the bilateral movements of health professionals, a gravity model is applied. The latter approach has been used in a number of studies (e.g. Landesmann, Mara and Vidovic 2015; Mara 2020) to analyse the mobility not just of the overall population but also of health professionals (Botezat and Ramos 2020). At the international level, gravity models have also been used for analysing the mobility of health professionals (Adovor et al. 2020; Beine, Bertoli and Fernández-Huertas Moraga 2016; Botezat and Ramos 2020). The rationale of a gravity framework is that an individual chooses to move abroad or not depending on his/her expectations about employment opportunities or the level of earnings in his/her country of origin in comparison with other countries. Apart from economic determinants, other time-invariant determinants which might facilitate mobility can be taken into account, such as geographical proximity or cultural and language affinities.
In the context of health professionals, by applying the gravity model we aim to capture the push-and-pull factors of mobility for the particular group of medical doctors. Expectations about employment opportunities outside the home country or a host country’s absorption capacity to retain or attract health professionals are recognised as important pull factors for the mobility of this group of workers. Higher earnings in this sector in a potential host country and relatively high wage differentials between sending and host countries are expected to have a positive impact on attracting health professionals to the potential host countries. Further, the demand for health professionals is expected to be driven by the health-service needs of the population. As outlined above, an ageing population certainly has a greater need for healthcare. Therefore, the demographic structure of the population and their differences across countries are expected to be important drivers of demand for health professionals. Countries where the demand for such personnel is high and the available financial resources are more abundant – e.g. for employing or offering a higher level of compensation to health professionals – tend to be more successful at retaining domestically trained doctors as well as attracting foreign-trained health professionals than countries which have financial constraints or offer lower wages in this sector.
Apart from the demand side, the supply side also matters. The supply of health professionals – for example, medical doctors – depends on the contingent of students and health graduates who join the labour market of health professionals. Therefore, we take into account these aspects of the demand-and-supply side of health professionals when estimating the gravity model.
The approach adopted in this study is first to analyse the push and pull factors of mobility in the context of a wider set of countries, namely the European and Western Balkan countries. The purpose here is first to estimate the effects of different push-and-pull factors of mobility and how robust they are for different set of countries, while controlling for origin and destination countries’ fixed effects. Secondly, as we are more interested in analysing the push-and pull-factors of mobility in the context of WB countries, a subset of estimates are performed having the individual European countries as the main destination countries and WB countries as the sending countries. Lastly, we are interested in accounting for the effect of recent policy changes, such as the free visa regime and the Western Balkan employment regulation introduced in Germany in 2016. Therefore, further specifications will be estimated where the policy-change effects are captured by respective dummies for such policies.
Because of data availability, the gravity model for health professionals’ mobility can be estimated using only the OECD statistics with respect to medical doctors, at pair-country level between European and Western Balkan countries and for the 2001–2019 period. The econometric approach applied here is similar to the one applied by Botezat and Ramos (2020). The estimated equation is defined as follows:
eq. (1)

whereby the main determinants are:
 – the dependent variable – refers to the stock of foreign doctors residing in destination country (f) and originating from country (i), and
– the dependent variable – refers to the stock of foreign doctors residing in destination country (f) and originating from country (i), and  accounts for the migration stock and network effects of health professionals (in this case medical doctors) for attracting health professionals from a given sending country (i) to a given destination (f). The choice of using stock data instead of flow data was motivated by the fact that flow data showed poor quality, especially in the context of Western Balkan countries. The information about inflow of medical doctors presented many missing data points. In contrast, stock data revealed fewer missing data points than flow data. For this reason, we used stock data to have more data points and consequently use more accurate observations for estimating the gravity model.
accounts for the migration stock and network effects of health professionals (in this case medical doctors) for attracting health professionals from a given sending country (i) to a given destination (f). The choice of using stock data instead of flow data was motivated by the fact that flow data showed poor quality, especially in the context of Western Balkan countries. The information about inflow of medical doctors presented many missing data points. In contrast, stock data revealed fewer missing data points than flow data. For this reason, we used stock data to have more data points and consequently use more accurate observations for estimating the gravity model.- We also control for a number of time-variant variables presented by vector X – specifically we have included a number of variables which could be important push-and-pull factors of mobility such as:
- wage rates in the health sector in the destination and origin country,
 and
and  respectively (given that data on doctors’ levels of earnings are not available, we use health-sector levels of earnings as a proxy5), as well as the gaps in income level between the sending and the destination country of health professionals captured by the ratio of GDP per capita in purchasing power parity (PPP) between sending and receiving countries;
respectively (given that data on doctors’ levels of earnings are not available, we use health-sector levels of earnings as a proxy5), as well as the gaps in income level between the sending and the destination country of health professionals captured by the ratio of GDP per capita in purchasing power parity (PPP) between sending and receiving countries; - the density of medical doctors per 10,000 inhabitants in the origin and sending countries as a proxy for the supply of medical doctors in the respective origin and destination countries;
- the share of health graduates in the respective foreign country and the country of origin as a proxy for the supply of health professionals;
- the share of the population aged 65+ in the respective foreign country and the country of origin as a proxy for the demand for health professionals.
- wage rates in the health sector in the destination and origin country,
- Other determinants, which are country-pair specific and constant over time, are represented by:
 , the geographical distance between the sending and host country;
, the geographical distance between the sending and host country; , sharing a border;
, sharing a border; which refers to sharing the same official language.
which refers to sharing the same official language.
- We also control for a number of policy changes in Europe which are considered relevant in the context of WB countries – such as a free visa regime and the WB employment regulation introduced in Germany in 2015 targeting migrants from WB countries.
Data and descriptive statistics
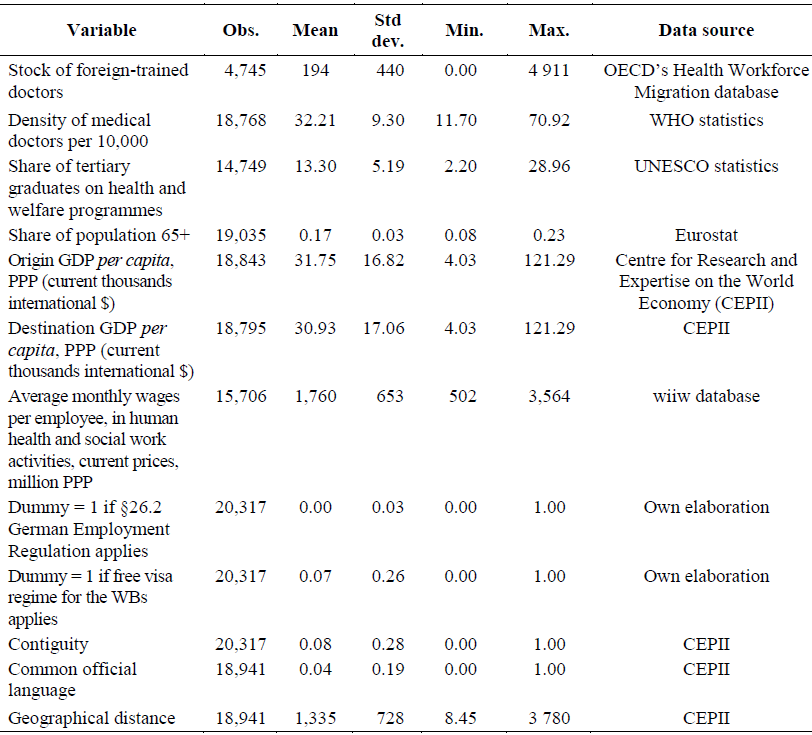
Several data sources have been used to empirically estimate the gravity model for the mobility of health professionals. Statistics for their bilateral mobility were obtained from the OECD’s Health Workforce Migration database for the category of medical doctors. Data concerning the bilateral stock of medical doctors by country of origin in the OECD are available for the period 2001–2019 or the latest year available. For this analysis I used a selected number of OECD countries. The sample is composed of European destination countries, whereas the European and the WBs have been selected as the main sending countries. Other indicators, such as the density of the body of medical doctors, were obtained from World Health Organisation (WHO) Statistics. The shares of tertiary graduates on health and welfare programmes were obtained from the United Nations Educational, Scientific and Cultural Organization (UNESCO) statistics. The shares of the population above the age of 65 were obtained from Eurostat and those on the remuneration of health professionals from the wiiw database, which uses national accounts data to calculate monthly wages in the health sector, both in euros and in purchasing power parity (PPP). The gravity variables, such as distance, common ethnic language and contiguity/common border as well as the GDP per capita in PPP were obtained from the Centre for Research and Expertise on the World Economy (CEPII). Table 2 presents some basic descriptive statistics on the main variables used for the gravity model estimation.
Estimation results of the gravity model
In this section, two sets of estimation results are presented. The first are the results attained by estimating the gravity model for a large set of countries where both sending and destination countries are represented by European and Western Balkan countries. The European countries are represented by the EU28, Switzerland and Norway and the WB countries by Albania, Bosnia and Herzegovina, Montenegro, North Macedonia and Serbia. The results are presented in Table 3. In the second set of results, the gravity model is estimated in a subset of countries with the WB countries as the sending countries and European countries as the destination countries. In this subset of estimates, further specifications have been included which aim to capture the effects of policy changes. Furthermore, for robustness checks, other specifications for this subset of countries have been estimated and are presented in Table 4, to be discussed later.
Table 2. Descriptive statistics used for the gravity model, 2000–2019
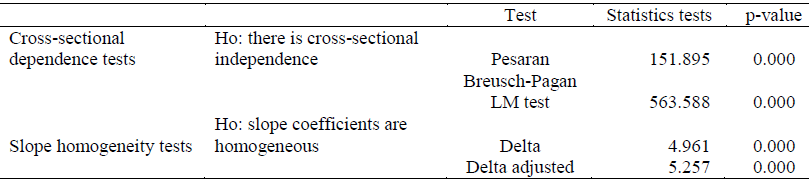
As was highlighted above, the empirical analysis aims to establish the main determinants of medical doctors’ mobility in a general context and then, more specifically, in the context of WB countries. The general model of medical doctors’ mobility is tested empirically by running the gravity model for a wide set of countries, where the dependent variable is the stock of migrants at pair-country level between WB and European countries. Since we want to account for both time-variant and time-invariant determinants, we apply OLS regressions. For the model selection we also run a few diagnostic tests such as slope homogeneity and cross-section independence of the error terms. The first test is relevant for understanding whether the effects of the parameters of interest are constant or vary across countries. Especially in this context, where we are dealing with a large set of countries – at least 35 countries, at pair-country level and for a long time series – 2001–2019 – it is very likely that cross-section dependence can be an issue which, if it is not addressed properly, might generate inconsistent estimates. The respective tests presented in Annex Table A1 indicate that we have a cross-sectional dependence in the data. To correct for this, the model has been estimated by running pooled OLS/WLS with Driscoll and Kraay standard errors following Hoechle (2007). The advantage of this approach is that it allows for the error terms to be heteroskedastic and robust to cross-section dependence.
The estimation results in Table 3 show a positive significant sign with respect to the lagged stock of foreign-trained doctors and indicate their robustness across different specifications, accounting for the different fixed effects. This result suggests the importance of networks among health professionals in a given destination country for attracting other doctors from a given origin country. The results also indicate that variables which are time invariant – such as contiguity and geographical distance between countries – do matter and explain the mobility. For the European countries (Table 3) in particular, the contiguity and sharing of a common border positively affects the mobility of medical doctors; whereas, with increasing geographical distance, the mobility of medical doctors to other, further destinations is less likely to occur.
Table 3. Determinants of medical doctors’ mobility: gravity model estimates for Europe and WBs at pair country level, 2001–2019
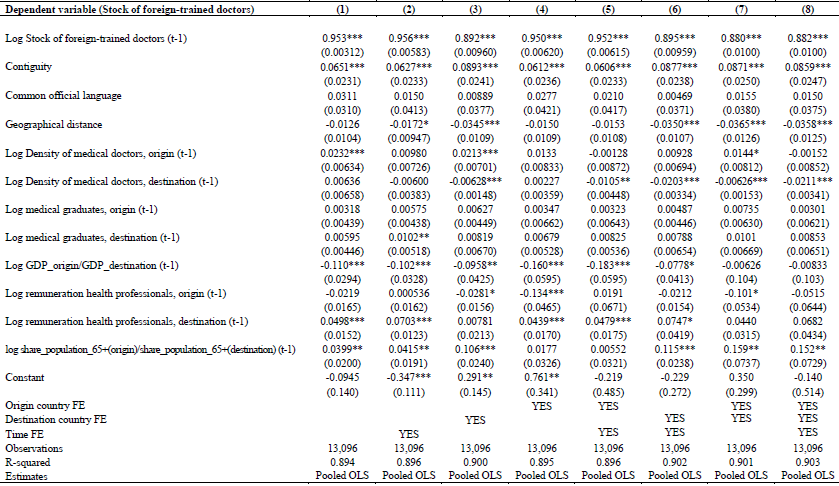
Notes: Standard errors in parentheses; + p < 0.10, * p < 0.05, ** p < 0.01, *** p < 0.001.
With regards to the estimation results about the density of the stock of medical doctors, we find that origin countries with a higher-density stock are likely to experience a larger body of migrants abroad, although the result is not robust across all the specifications. In contrast, the stock of foreign-trained doctors has a negative relationship with the medical doctor stock density in the destination country, implying that, with the rise of the stock of medical doctors in the destination country, that of foreign-trained doctors is reduced – a result which might be explained as a lower demand for foreign-trained doctors if domestic supply is rather high.
Regarding the estimation results about the remuneration of health professionals and how it affects their mobility, we observe a positive and significant relationship concerning the receiving-country wages; the results seem to hold, especially if we account for destination countries’ fixed effects. A relatively higher level of earnings in the receiving country attracts more medical doctors from abroad. At the same time, we find a negative and significant coefficient concerning the origin-country wages, which suggests that higher wages in the domestic market might deter the outward mobility of medical doctors, when both origin- and destination-country fixed effects are counted. Therefore, countries which tend to have a higher remuneration of health professionals attract more health professionals from abroad. However, from the perspective of the sending countries, it is also true that higher wages at home might be accompanied by a lower number of medical doctors moving abroad. Therefore, remuneration in the health sector might be a strong pull factor to emigrate but might also deter the outward migration of health-sector workers. In terms of the size of coefficients, an increase in the remuneration at home of 10 per cent might deter the stock of doctors moving abroad by 10 per cent. While looking at the income gap in the origin and destination country, proxied by the level of GDP per capita in PPP, the results suggest that a higher income ratio – which implies the narrowing of the income gap between sending and receiving countries – for example with 10 per cent – would reduce emigration of health professionals.
With respect to the demand-side determinants, the results suggest a positive relationship of the ratio of the population share aged 65+ between sending and destination country and the stock of foreign-trained doctors. The positive sign of the coefficient suggests that the higher the gap in terms of the population aged 65+ between the origin and the destination country, the more likely we are to see doctors moving from origin to destination countries, which is explained by a higher demand for medical doctors for the latter owing to their higher share of the population aged 65+.
Estimation results of the gravity model for the Western Balkan countries
The second set of estimation results for the Western Balkan countries are presented in Table 4. The first specification has been estimated by running pooled OLS/WLS with Driscoll and Kraay standard errors following Hoechle (2007). In addition, for the robustness check, the model for the subset of WB countries has been estimated by running the Poisson pseudo maximum likelihood (PPML). When estimating gravity models with a large set of countries, one shortcoming which is often encountered is the probable high number of zeros or missing information for several indicators, either flow or stock data. Moreover, the log transformation of zero values among the observations further enlarges the sample of missing information. Therefore, estimating the model for the subset of WB countries using the Poisson pseudo maximum likelihood (PPML) allows me to account for the large number of zeros and to cross-check the validity of the estimates (Santos Silva and Tenreyro 2010). Accordingly, in the PPML regressions, the errors are clustered at the pairing-country level. The results of the OLS and PPML are presented in Table 4.
Table 4. Determinants of medical doctors’ mobility from WB to Europe, 2001–2019
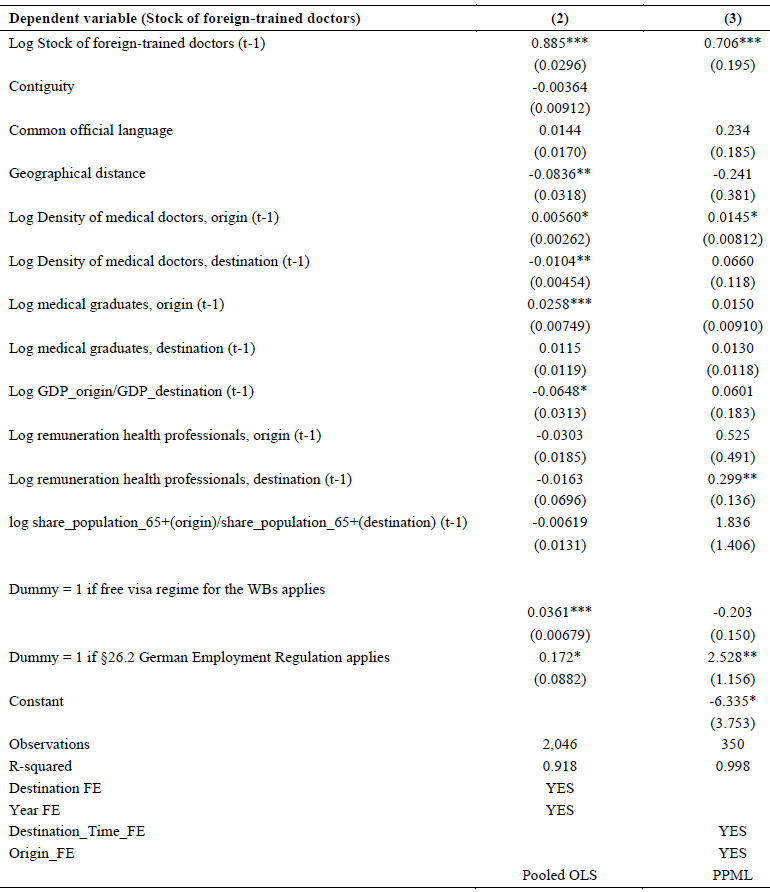
Notes: Standard errors in parentheses; + p < 0.10, * p < 0.05, ** p < 0.01, *** p < 0.001.
The estimation results confirm the importance of networks in a destination country for attracting other doctors from a given origin country. Among time-invariant variables, the geographical distance matters and negatively effects the outward mobility of medical doctors. Once again, the supply of medical doctors, including graduates, seems to be positively associated with the stock of doctors abroad. Particularly for the WB countries, the results suggest that a high share of health graduates is positively related with outward migration. The explanations for these results might be related to an excessive supply of medical doctors or the somewhat weak absorption capacity of health professionals by the domestic labour market, which might push the emigration of this category of workers.
With respect to the remuneration of medical doctors, we find that the income gap is an important driver of outward mobility for this group. In the context of WB countries, the results suggest that the narrowing of the income gap between sending and receiving countries – for example by 10 per cent – would reduce the emigration of medical doctors by 6.5 per cent.
With respect to the migration policy changes which encourage the mobility of people, together with changes in the migration regime which facilitate mobility for a particular group of countries – such as the WB Employment Regulation in Germany – the results indicate that the latter regulation has been quite an important pull factor for the migration of medical doctors from the WBs. The results are robust across specifications and the impact seems to have been stronger than the network effect. The emigration of medical doctors from the WBs has risen by almost 10 per cent due to this new regulation. These results emphasise the importance of mobility programmes and migration regime changes and their role for mobility, in this case of medical doctors. In the context of WB countries, the outward mobility of medical doctors had been driven by the remuneration of health professionals and facilitated by the new regulation of emigrants from the WBs in Germany, hinting that their mobility is both supply- and demand-driven. Domestic factors, however, are shown to be less relevant, though higher wages would deter outward mobility.
Main findings and conclusions
This study has analysed the patterns of mobility of health professionals across European countries with a specific focus on medical doctors from the Western Balkans. The paper first presented a number of stylised facts to sketch the demand and supply of health professionals and the role that their mobility has played in satisfying the demand for this category of workers across European countries. This overview found that, among EU countries, there are diverging patterns as far as both the demand and the supply of health professionals are concerned. A number of countries have managed to satisfy their demand by recruiting foreign-trained health professionals. The battle for health professionals among EU countries has produced both winners and losers. This implies that, for a group of countries – especially those from the EU-CEE and Western Balkan countries, which are mainly net senders of health professionals – severe drawbacks to their mobility prevail.
To better understand the drivers of mobility, a gravity model was estimated for the mobility of medical doctors covering European and WB countries over the period 2000–2019. This found that the prospect of better earnings and higher wage gaps between health professionals across Europe are certainly important drivers of the mobility of medical doctors. Geographical proximity and contiguity are relevant for explaining the mobility of health professionals from within Europe and for the WBs.
On the supply side, from the perspective of the destination country, a higher number of graduate health professionals might be accompanied by a lower dependence on health professionals from abroad. In contrast, from the perspective of the sending country, we might associate this with a higher supply of health professionals being sent abroad, which hints at low absorption capacities in the sending countries of medical doctors especially in the case of the WB countries.
On the demand side, the results confirm that, here, the mobility of health professionals does play a role. In particular, the age structure of the population and, consequently, the demand for long-term care, is driving the mobility of doctors from the perspective of both the sending and the destination country, though the results are not confirmed for the WB countries.
Foreign-trained doctors, by and large, tend to complement the demand for health professionals; network effects also matter and are an important determinant of mobility among medical doctors. Furthermore, new changes in the regulations which manage migration and the employment of migrants from the WBs in general – such as that introduced by Germany in 2015 – are attracting more and more health professionals from the WBs to Germany.
New policy measures in the countries of origin – the WBs – or bilateral agreements between sending and destination countries, need to be introduced, with the aim of balancing the mobility of health professionals such that the demand for them is satisfied in both the sending and the destination country. Furthermore, this must be combined with rising wages for this category of health professional in order to deter their outward mobility. Besides, what seems to matter for the mobility of medical doctors in general and, in particular, for the WB countries, are not only higher wages in the destination country but also a higher standard of living and quality of life.
The circular migration of health professionals or short-term exchange programmes between countries might be a much more effective approach. Already the WB region has produced high rates of outward mobility, including that of health professionals. Therefore, a further intensification of outward mobility for this category of workers might be devastating for the region. Also, skill development and mobility programmes such as those offered by Germany in the WBs – the Dekra Academy and Heimerer College (ETF 2022) – are desirable but should be better regulated and assure a balanced supply of health professionals for the domestic and foreign market.
Funding
No funding was provided during the preparation of this study. However, the study greatly benefited from the work and funding obtained within the framework of ETF and BMASGK projects (ETF project – https://wiiw.ac.at/migration-and-human-capital-in-the-western-balkans-pj... BMASGK project – https://wiiw.ac.at/arbeei-international-grundlagen-und-angewandte-arbeit...).
Conflict of interest statement
No conflict of interest was reported by the author.
ORCID ID
Isilda Mara  https://orcid.org/0000-0002-2598-2333
https://orcid.org/0000-0002-2598-2333
Notes
- For the purposes of this article, the WBs include Albania, Bosnia and Herzegovina, Montenegro, North Macedonia and Serbia. There were not sufficient data for Kosovo to be included in the analysis, except where otherwise specified.
- The so-called ‘Western Balkan Regulation’ (§26.2 German Employment Regulation) was introduced to: (i) create a legal pathway to migrate to Germany and reduce the number of irregular migrants and asylum-seekers from the WB6; (ii) provide access to labour migrants from the WB6 regardless of their skill level; and (iii) meet labour market needs in Germany – both for low- and high-skilled workers in sectors affected by labour shortages (ETF 2022).
- This study partly draws from two other studies conducted by the author within the framework of the ETF and BMASGK projects, and it partly draws from the previously issued online reports. For details, see ETF project – https://wiiw.ac.at/migration-and-human-capital-in-the-western-balkans-pj... BMASGK project – https://wiiw.ac.at/arbeei-international-grundlagen-und-angewandte-arbeit....
- For this analysis, ‘Europe’ is defined as the EU28, plus Norway and Switzerland.
- Health professionals’ remuneration, defined as the average monthly wages per employee, in human health and social work activities, are provided in current prices, in million PPP.
References
Adovor E., Czaika M., Docquier F., Moullan Y. (2020). Medical Brain Drain: How Many, Where and Why? Journal of Health Economics 76: 102409.
Beine M., Bertoli S., Fernández-Huertas Moraga J. (2016). A Practitioners’ Guide to Gravity Models of International Migration. World Economy 39(4): 496–512.
Botezat A., Ramos R. (2020). Physicians’ Brain Drain: A Gravity Model of Migration Flows. Globalization and Health 16(1): 7.
Brücker H., Falkenhain M., Fendel T., Promberger M., Raab M., Trübswetter P., Blažević L., Trmkoli M. (2020). Evaluierung der Westbalkanregelung: Registerdatenanalyse und Betriebsfallstudien: Abschlussbericht. Berlin: Bundesministerium für Arbeit und Soziales.
Buchan J., Campbell J., Dhillon I., Charlesworth A. (2019). Labour Market Change and the International Mobility of Health Workers. London: The Health Foundation Working Paper No. 5.
CEDEFOP (2018). Skills Panorama. Thermi: European Centre for the Development of Vocational Training.
Davda L.S., Gallagher J.E., Radford D.R. (2018). Migration Motives and Integration of International Human Resources of Health in the United Kingdom: Systematic Review and Meta-Synthesis of Qualitative Studies Using Framework Analysis. Human Resources for Health 16(1): 1–13.
European Commission (2017). A Comparison of Shortage and Surplus Occupations Based on Analyses of Data from the European Public Employment Services and Labour Force Surveys, Bottleneck Occupations 2016. Brussels: European Commission, Directorate-General for Employment, Social Affairs and Inclusion.
ETF (2022). ‘Use It, or Lose It’. How Do Migration, Human Capital and the Labour Market Interact in the Western Balkans? Turin: European Training Foundation.
Glinos I. (2015). Health Professional Mobility in the European Union: Exploring the Equity and Efficiency of Free Movement. Health Policy 119(12): 1529–1536.
Grignon M., Owusu Y., Sweetman A. (2013). The International Migration of Health Professionals, in: A.F. Constant, K.F. Zimmermann (eds), International Handbook on the Economics of Migration, pp. 75–97. Cheltenham: Edward Elgar.
Hoechle D. (2007). Robust Standard Errors for Panel Regressions with Cross-Sectional Dependence. The Stata Journal 7(3): 281–312.
Kroezen M., Dussault G., Craveiro I., Dieleman M., Jansen C., Buchan J., Barriball L., Rafferty A.M., Bremner J., Sermeus W. (2015). Recruitment and Retention of Health Professionals across Europe: A Literature Review and Multiple Case Study Research. Health Policy 119(12): 1517–1528.
Landesmann M., Mara I., Vidovic H. (2015). SEE 2020 Strategy: Study on Labour Mobility. Vienna: Vienna Institute for International Economic Studies, wiiw Research Report No. 408.
Liu J.X., Goryakin Y., Maeda A., Bruckner T., Scheffler R. (2017). Global Health Workforce Labor Market Projections for 2030. Human Resourses for Health 15(11): 1–12.
Maeda A., Socha-Dietrich K. (2021). Skills for the Future Health Workforce: Preparing Health Professionals for People-Centred Care. Paris: OECD Health Working Paper No. 124.
Mara I. (2019). Doctors on the Move: Mobility Patterns in the EU. Vienna: Vienna Institute for International Economic Studies, wiiw Monthly Report No. 7–8.
Mara I. (2020). Health Professionals Wanted: Chain Mobility across European Countries. Vienna: Vienna Institute for International Economic Studies, wiiw Research Report No. 445.
Mullan F. (2005). The Metrics of the Physician Brain Drain. New England Journal of Medecine 353(17): 1810–1818.
OECD (2015). International Migration Outlook 2015. Paris: Organisation for Economic Cooperation and Development.
OECD (2019a). OECD Health Statistics 2019 Online Database. Paris: Organisation for Economic Cooperation and Development.
OECD (2019b). Recent Trends in International Migration of Doctors, Nurses and Medical Students. Paris: Organisation for Economic Cooperation and Development.
Ognyanova D., Maier C.B., Wismar M., Girasek E., Busse R. (2012). Mobility of Health Professionals Pre and Post 2004 and 2007 EU Enlargements: Evidence from the EU Project PROMeTHEUS. Health Policy 108(2–3): 122–132.
Santos Silva J.M.C., Tenreyro S. (2010). On the Existence of the Maximum Likelihood Estimates in Poisson Regression. Economics Letters 107(2): 310–312.
Scarpetta S., Dumont J.C., Socha-Dietrich K. (2020). Contribution of Migrant Doctors and Nurses to Tackling the COVID-19 Crisis in OECD Countries. Paris: Organisation for Economic Cooperation and Development.
Scheffler R.M., Campbell J., Cometto G., Maeda A., Liu J., Bruckner T.A., Arnold D.R., Evans T. (2018). Forecasting Imbalances in the Global Health Labor Market and Devising Policy Responses. Human Resources for Health 16(1): 1–10.
Schultz C., Rijks B. (2014). Mobility of Health Professionals to, from and within the European Union. New York: United Nations, IOM Migration Research Series No. 48.
Schmitz-Pranghe C., Oruč N., Mielke K., Ibričević A. (2020). Making Sure that the Emigration of Healthcare Personnel from Albania and BiH Works for All: What Germany Can Do. Bonn: Bonn International Centre for Conflict Studies, BICC Policy Brief 8.
Tjadens F., Weilandt C., Eckert J. (2012). Mobility of Health Professionals: Health Systems, Work Conditions, Patterns of Health Workers’ Mobility and Implications for Policy Makers. Berlin and Heidelberg: Springer Science & Business Media.
Williams G.A., Jacob G., Rakovac I., Scotter C., Wismar M. (2020). Health Professional Mobility in the WHO European Region and the WHO Global Code of Practice: Data from the Joint OECD/EUROSTAT/WHO-Europe Questionnaire. European Journal of Public Health 30(Supplement 4): iv5-iv11.
Wismar M., Maier C.B., Glinos I.A., Bremner J., Dussault G., Figueras J. (2011). Health Professional Mobility and Health Systems in Europe: An Introduction. Brussels: European Observatory on Health Systems and Policies.
WHO (2022). Seventy-Fifth World Health Assembly Provisional Agenda Item 15 (A75/12): Human Resources for Health: Working for Health: Draft – 2030 Action Plan. Report by the Director-General. https://www.who.int/news/item/02-06-2022-from-resolution-to-action-high-... (accessed 5 December 2023).
World Bank Group, Vienna Institute for International Economic Studies (2018). Western Balkans Labor Market Trends 2018. https://wiiw.ac.at/western-balkans-labor-market-trends-2018-dlp-5169.pdf (accessed 6 December 2023).
Annex 1
Table A1. Diagnostic tests
Copyright information
© The Author(s)
Open Access
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.